AIM: Determination of Total Cholesterol
Introduction
-
Total cholesterol is the total amount of cholesterol present in blood, including LDL, HDL, and VLDL fractions.
-
It is an essential lipid required for cell membrane structure, steroid hormone synthesis, bile acid formation, and vitamin D production.
-
Determination of total cholesterol is important for assessing the risk of cardiovascular diseases and diagnosing lipid disorders.
-
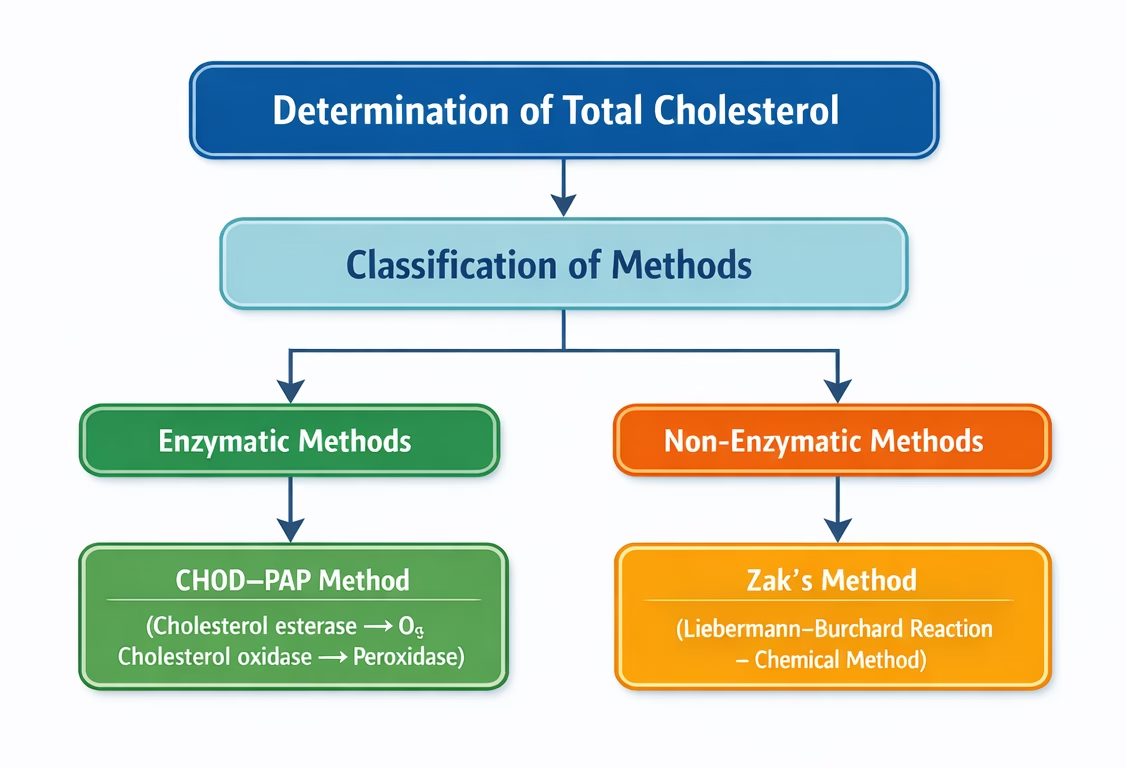
It is commonly estimated by the enzymatic CHOD-PAP method, where color intensity produced is directly proportional to cholesterol concentration.
-
The normal desirable serum cholesterol level in adults is less than 200 mg/dL.
Principle of an enzymatic method
The enzymatic method for determination of total cholesterol is based on sequential enzymatic reactions that produce a colored compound. The intensity of the color formed is directly proportional to the cholesterol concentration in the sample.
- Cholesterol ester + H2O ————>Cholesterol esterase —————> Cholesterol + Fatty acids
- Cholesterol + O2 —————->Cholesterol oxidase —————–> Cholesterol-4-en-3-one + H2O2
- 2H2O2+ 4-aminoantipyrine + Phenol ———-> Peroxidase ————> Quinoneimine dye + 4H2O
Sample
- Serum or plasma (collected after 12–14 hours of fasting for accurate results).
- Preparation of PFF (Protein filtrate) from serum.
- Take 9.9 ml ferric chloride
- Acetic acid reagent in a dry test tube
- 0.1 ml serum (Dilution of blood = 1 in 100).
- Mix by inversion using paraffin film, keep for 5 minutes, centrifuge, and use clear supernatant as PFF.
Reagents Composition
| R1 | |
| Good’s Buffer | 50 mmol/l |
| Phenol | 5 mmol/l |
| 4-aminoantopyrine | 0.3 mmol/l |
| Cholesterol esterase | > 200 U/l |
| Cholesterol oxidase | > 50U/l |
| Peroxidase | > 3 kU/l |
| R2 Standard | — |
Procedure
| Test | Standard | Blank | |
| Reagents 1 | 1.00 ml | 1.00 ml | 1.00 ml |
| Sample | 0.01 ml | – | – |
| Standard | – | 0.01 ml | – |
| Distilled water | – | – | 0.01 ml |
Principle Zak’s Method
- Cholesterol in the serum reacts with acetic anhydride and concentrated sulfuric acid in the presence of ferric chloride.
- This reaction produces a green-colored complex due to the formation of cholestadiene derivatives.
- The intensity of the green color formed is directly proportional to the concentration of cholesterol present in the sample.
- The color intensity is measured colorimetrically at approximately 540–560 nm. (green filter).
Reagents
- 05 g ferric chloride hexahydrate in acetic acid,
- H2SO4.
- Standard cholesterol solution: (5 ml ≡ 0.2 mg cholesterol), prepared fresh in ferric chloride—acetic acid reagent from stock cholesterol solution (100 mg/100 ml acetic acid).
Procedure
| Test | Standard | Blank | |
| PFF | 5 ml | – | – |
| Standard cholesterol solution | – | 5 ml | – |
| Ferric chloride-acetic acid reagent | – | – | 5 ml |
| Conc. H2SO4 | 3 ml | 3 ml | 3 ml |
Calculation
The concentration of total cholesterol in the sample is calculated using the formula:
Cholesterol concentration (mg/dL) = Sample Absorbance / Standard Absorbance × Standard Concentration (mg/dl)
Normal Values
The normal range of total cholesterol depends on age, sex, and other factors. General reference ranges are:
- Desirable: < 200 mg/dL (5.2 mmol/L)
- Borderline High: 200–239 mg/dL (5.2–6.2 mmol/L)
- High: ≥ 240 mg/dL (6.2 mmol/L)
Age-Specific Reference Ranges:
- Children: 120–170 mg/dL
- Adults: 140–200 mg/dL
- Elderly (>65 years): Up to 220 mg/dL may be normal.
Clinical Significance
Elevated Total Cholesterol
High cholesterol levels (hypercholesterolemia) are a key risk factor for cardiovascular diseases. Causes include:
- Primary hyperlipidemia (genetic):
- Familial hypercholesterolemia.
- Familial combined hyperlipidemia.
- Secondary hyperlipidemia (acquired):
- A diet high in saturated fats and cholesterol.
- Hypothyroidism.
- Diabetes mellitus.
- Nephrotic syndrome.
- Obstructive liver disease.
- Chronic kidney disease.
Clinical Implications:
- Atherosclerosis: Plaque buildup in arteries leading to reduced blood flow.
- Coronary artery disease: Increased risk of heart attacks.
- Stroke: Higher chances of ischemic stroke due to arterial blockages.
Decreased Total Cholesterol
Low cholesterol levels (hypocholesterolemia) are less common but may indicate:
- Malnutrition or malabsorption.
- Hyperthyroidism.
- Liver diseases (e.g., cirrhosis or liver failure).
- Chronic infections or inflammation.
- Severe anaemia.
Clinical Implications:
- Reduced steroid hormone synthesis.
- Weak immunity due to insufficient cell membrane production.
- Neurological disorders (rare cases linked to low cholesterol).