Introduction
-
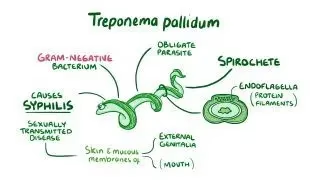
Treponema species are thin, spiral-shaped bacteria belonging to the family Spirochaetaceae.
-
Among them, Treponema pallidum is the most medically important species and is the causative agent of syphilis.
-
Syphilis is a chronic, systemic sexually transmitted infection with multiple clinical stages and diverse manifestations.
-
Other pathogenic treponemes such as T. pertenue and T. carateum cause non-venereal diseases like yaws and pinta.
-
Treponema species are highly fastidious organisms and cannot be cultured on routine laboratory media.
-
Their unique morphology, motility, and immune evasion mechanisms contribute to persistent infection.
-
Laboratory diagnosis relies mainly on direct microscopy and serological tests.
-
Treponemal infections remain a significant global public health problem, especially in developing countries.
General Character
Genus: Treponema
Taxonomic Classification
-
Genus: Treponema
-
Family: Spirochaetaceae
Medically Important Species
-
Treponema pallidum – Causes syphilis
-
Treponema pertenue – Causes yaws
-
Treponema carateum – Causes pinta
These species are collectively referred to as pathogenic treponemes and are responsible for chronic human infections.
Morphological Characteristics
Gram Staining
-
Treponema species are Gram-negative
-
Due to their extremely thin structure and delicate peptidoglycan layer, they are not easily visualized by routine Gram staining
-
Special techniques such as dark-field microscopy or silver impregnation stains are required
Shape and Arrangement
-
Shape: Spiral-shaped bacteria (spirochetes)
-
Arrangement:
-
Usually present as single organisms
-
Occasionally may appear in small clusters under microscopy
-
-
Exhibit characteristic corkscrew motility, which aids tissue penetration
Oxygen Requirement
-
Treponema species are anaerobic or microaerophilic
-
They thrive in low-oxygen environments, such as:
-
Subcutaneous tissues
-
Mucous membranes
-
Lymphatic and vascular systems
-
Morphology
Treponema species are delicate, slender, spiral-shaped bacteria belonging to the spirochetes. Their unique morphology plays a crucial role in their motility and pathogenicity.
Size
-
Length: 6–15 µm
-
Diameter: ~0.1–0.2 µm
-
Extremely thin compared to other bacteria
Shape
-
Spiral-shaped (spirochete)
-
Possess tight, regular, and uniform coils
-
Ends are pointed and tapering
Arrangement
-
Usually found as single, free-living organisms
-
Rarely seen in chains or clusters
Cell Structure
-
Gram-negative in nature, but poorly stained with routine Gram stain
-
Cell envelope consists of:
-
Outer membrane with few exposed proteins
-
Thin peptidoglycan layer
-
Cytoplasmic membrane
-
This unique structure contributes to low antigenicity and immune evasion.
Motility
-
Highly motile with corkscrew or screw-like movement
-
Motility is due to periplasmic flagella (axial filaments) located between the cell wall and outer membrane
-
Enables penetration through viscous media and tissues
Staining Characteristics
-
Not visualized by:
-
Gram stain
-
Ziehl–Neelsen stain
-
-
Best demonstrated by:
-
Dark-field microscopy
-
Phase-contrast microscopy
-
Silver impregnation methods (Warthin–Starry stain)
-
Direct fluorescent antibody (DFA) tests
-
Special Morphological Features
-
Fragile organism, easily destroyed by:
-
Heat
-
Drying
-
Disinfectants
-
-
Does not form spores
-
No capsule
Cultural Characteristics
Growth on Artificial Media
-
Treponema pallidum cannot be cultured on routine or artificial laboratory media
-
No growth on:
-
Blood agar
-
Chocolate agar
-
MacConkey agar
-
-
This is due to:
-
Lack of essential metabolic pathways
-
Dependence on host cells for nutrients
-
Growth in Experimental Animals
-
Can be maintained only in living tissue
-
Commonly propagated in:
-
Rabbit testes (standard experimental model)
-
-
Used mainly for:
-
Research purposes
-
Antigen preparation
-
Pathogenesis studies
-
Oxygen Requirement
-
Anaerobic to microaerophilic
-
Requires low oxygen tension for survival
-
Does not survive well in aerobic laboratory conditions
Temperature and Environmental Sensitivity
-
Optimal survival near 37°C
-
Highly sensitive to:
-
Heat
-
Drying
-
Soap and disinfectants
-
-
Rapidly loses viability outside the host
Metabolic Characteristics
-
Limited metabolic activity
-
Utilizes host-derived nutrients
-
Does not produce many detectable biochemical reactions
Biochemical Reactions
General Biochemical Characteristics
-
Biochemically inert organism
-
Shows minimal enzymatic and metabolic activity
-
Lacks many metabolic pathways necessary for independent survival
-
Highly dependent on host cells for nutrients and energy
Carbohydrate Utilization
-
Does not ferment carbohydrates in standard laboratory tests
-
Energy is obtained mainly from host-derived glucose and amino acids
-
No detectable acid or gas production in routine media
Enzyme Activity
-
Catalase: Negative
-
Oxidase: Negative
-
Urease: Negative
-
Indole: Negative
Routine enzymatic tests are not useful for laboratory identification.
Protein and Amino Acid Metabolism
-
Limited ability to synthesize amino acids
-
Relies on host tissue for:
-
Amino acids
-
Fatty acids
-
Nucleotides
-
Lipid Metabolism
-
Cannot synthesize fatty acids efficiently
-
Utilizes host lipids for membrane formation
-
Outer membrane has few exposed proteins, contributing to low antigenicity
Pathogenicity
Virulence Factors of Treponema Species
1. Surface Proteins (Antigenic Variation)
-
Treponema pallidum possesses variable outer surface proteins
-
Continuous antigenic variation helps the organism:
-
Evade host immune response
-
Establish chronic and persistent infection
-
-
Low antigen density on the outer membrane delays immune recognition
2. Hyaluronidase
-
Enzyme produced by Treponema pallidum
-
Breaks down hyaluronic acid in connective tissue
-
Facilitates:
-
Tissue invasion
-
Rapid local spread
-
Hematogenous dissemination
-
Clinical Infections Caused by Treponema Species
1. Treponema pallidum – Syphilis
Syphilis is a chronic systemic disease with multiple clinical stages:
Primary Syphilis
-
Appearance of a painless, indurated chancre at the site of inoculation
-
Regional lymphadenopathy
-
Highly infectious stage
Secondary Syphilis
-
Due to systemic dissemination of organisms
-
Features include:
-
Generalized skin rash (palms and soles)
-
Mucous membrane lesions
-
Condylomata lata
-
Fever, malaise, and lymphadenopathy
-
Latent Syphilis
-
Asymptomatic phase
-
Serological tests remain positive
-
Divided into:
-
Early latent
-
Late latent
-
-
Disease may reactivate
Tertiary Syphilis
-
Occurs years after untreated infection
-
Severe complications include:
-
Gummatous lesions
-
Cardiovascular syphilis (aortitis, aneurysm)
-
Neurosyphilis (tabes dorsalis, general paresis)
-
2. Treponema pertenue – Yaws
-
Non-venereal treponemal infection
-
Transmitted by direct skin contact
-
Common in tropical and subtropical regions
-
Causes:
-
Chronic skin lesions
-
Bone and joint deformities in late stages
-
3. Treponema carateum – Pinta
-
Non-venereal treponemal disease
-
Primarily affects the skin
-
Characterized by:
-
Papular skin lesions
-
Progressive depigmentation
-
-
No systemic involvement
Laboratory Diagnosis
1. Specimen Collection
-
Exudate from chancre or mucous patches (primary/secondary syphilis)
-
Blood (serum) for serological tests
-
Cerebrospinal fluid (CSF) in suspected neurosyphilis
-
Placental tissue / cord blood in congenital syphilis
2. Direct Demonstration of the Organism
a. Dark-Field Microscopy
-
Specimen: Fresh exudate from chancre
-
Shows:
-
Thin, spiral-shaped, actively motile spirochetes
-
-
Most useful in early syphilis
-
Not useful for oral lesions (commensal spirochetes)
b. Direct Fluorescent Antibody Test (DFA-TP)
-
Uses fluorescein-labeled antibodies
-
Highly specific
-
Can differentiate pathogenic T. pallidum from non-pathogenic spirochetes
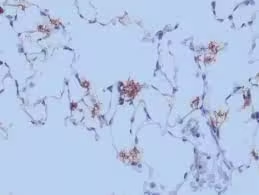
c. Silver Impregnation Staining
-
Warthin–Starry stain
-
Demonstrates spirochetes in tissue sections
-
Used mainly in histopathology
3. Serological Tests
Serology is the mainstay of diagnosis.
A. Non-Treponemal Tests (Screening Tests)
| Test | Principle | Use |
|---|---|---|
| VDRL | Detects reagin antibodies | Screening |
| RPR | Cardiolipin antigen test | Screening |
Advantages:
-
Inexpensive
-
Useful for monitoring treatment response
Limitations:
-
False positives
-
Less specific
B. Treponemal Tests (Confirmatory Tests)
| Test | Principle |
|---|---|
| TPHA | Hemagglutination |
| FTA-ABS | Fluorescent antibody test |
| ELISA | Detects treponemal antibodies |
Features:
-
Highly specific
-
Remain positive for life
-
Used for confirmation
4. CSF Examination (Neurosyphilis)
-
Elevated protein
-
Increased lymphocytes
-
Positive CSF-VDRL (highly specific)
5. Molecular Methods
-
PCR for detection of T. pallidum DNA
-
Useful in:
-
Early infection
-
Congenital syphilis
-
-
Limited availability
6. Diagnostic Algorithm
-
Screen with VDRL / RPR
-
Confirm with TPHA / FTA-ABS
-
Assess disease stage clinically
-
Monitor therapy with VDRL titers
Antibiotic Resistance
Susceptibility Pattern
-
Penicillin G remains the drug of choice for all stages of syphilis
-
No confirmed clinical resistance to penicillin has been documented
-
Treatment failure with penicillin is extremely rare and usually due to:
-
Inadequate dosing
-
Poor patient compliance
-
Reinfection
-
Resistance to Other Antibiotics
1. Macrolide Resistance
-
Increasing resistance reported to:
-
Azithromycin
-
Erythromycin
-
-
Resistance due to mutations in 23S rRNA gene
-
Leads to:
-
Treatment failure
-
Reduced usefulness of macrolides as alternative therapy
-
2. Tetracyclines
-
Doxycycline remains effective
-
Used in:
-
Penicillin-allergic patients
-
-
No widespread resistance reported, but requires strict compliance
3. Cephalosporins
-
Ceftriaxone shows good activity
-
Used in:
-
Neurosyphilis
-
Penicillin allergy (with caution)
-
Mechanisms Limiting Resistance Development
-
Lack of plasmids
-
Limited horizontal gene transfer
-
Reduced metabolic activity
-
Obligate dependence on host environment
Laboratory Detection of Resistance
-
Routine antimicrobial susceptibility testing is not feasible
-
Resistance detected by:
-
Molecular methods (PCR) identifying resistance-associated mutations
-
-
Surveillance studies guide treatment policies
Prevention
1. Primary Prevention (Preventing Infection)
Safe Sexual Practices
-
Consistent and correct use of condoms
-
Avoidance of:
-
Multiple sexual partners
-
Unprotected sexual intercourse
-
-
Sexual health education and awareness programs
Health Education
-
Public education regarding:
-
Modes of transmission
-
Early symptoms of syphilis
-
-
Promotion of responsible sexual behavior
-
Targeted education for high-risk populations
2. Secondary Prevention (Early Detection and Treatment)
Screening Programs
-
Routine serological screening for:
-
Pregnant women (antenatal screening)
-
Sexually active individuals at high risk
-
-
Early diagnosis prevents complications and transmission
Prompt Treatment
-
Early treatment with Penicillin G
-
Treatment of:
-
Infected individuals
-
Sexual partners (contact tracing)
-
3. Prevention of Congenital Syphilis
-
Mandatory antenatal screening during pregnancy
-
Immediate treatment of seropositive pregnant women
-
Follow-up testing of neonates born to infected mothers
4. Public Health Measures
-
Partner notification and treatment
-
Surveillance and reporting of cases
-
Accessible sexually transmitted infection (STI) clinics
-
Integration of syphilis control with HIV prevention programs
5. Infection Control Measures
-
Screening of blood donors
-
Use of sterile needles and syringes
-
Universal precautions in healthcare settings
6. Vaccination
-
No vaccine is currently available for syphilis
-
Prevention relies entirely on:
-
Behavioral modification
-
Screening
-
Early treatment
-
MCQs
1. Treponema pallidum belongs to which family?
A. Enterobacteriaceae
B. Spirochaetaceae
C. Mycobacteriaceae
D. Neisseriaceae
✅ Answer: B
2. The causative agent of syphilis is:
A. Treponema pertenue
B. Treponema carateum
C. Treponema pallidum
D. Borrelia burgdorferi
✅ Answer: C
3. Treponema species are best described as:
A. Gram-positive cocci
B. Gram-negative rods
C. Spiral-shaped spirochetes
D. Curved bacilli
✅ Answer: C
4. Routine Gram staining of Treponema pallidum is difficult because:
A. Thick capsule
B. Lack of cell wall
C. Extremely thin structure
D. Acid-fast nature
✅ Answer: C
5. Best method to visualize T. pallidum in early syphilis:
A. Gram stain
B. Ziehl–Neelsen stain
C. Dark-field microscopy
D. India ink
✅ Answer: C
6. Motility in Treponema pallidum is due to:
A. Polar flagella
B. Pili
C. Axial filaments
D. Cilia
✅ Answer: C
7. Oxygen requirement of Treponema species:
A. Obligate aerobe
B. Facultative anaerobe
C. Obligate anaerobe / microaerophilic
D. Capnophilic
✅ Answer: C
8. Treponema pallidum can be cultured on:
A. Blood agar
B. Chocolate agar
C. Lowenstein–Jensen medium
D. Cannot be cultured artificially
✅ Answer: D
9. Experimental animal used for propagation of T. pallidum:
A. Mouse
B. Guinea pig
C. Rabbit testes
D. Monkey
✅ Answer: C
10. Treponema pallidum is biochemically:
A. Highly active
B. Moderately active
C. Inert
D. Acid fermenter
✅ Answer: C
11. Catalase test for Treponema pallidum is:
A. Positive
B. Weakly positive
C. Variable
D. Negative
✅ Answer: D
12. Enzyme that facilitates tissue invasion in syphilis:
A. Coagulase
B. Hyaluronidase
C. Lecithinase
D. DNase
✅ Answer: B
13. Humans are the _____ host for T. pallidum:
A. Intermediate
B. Accidental
C. Only natural
D. Reservoir and vector
✅ Answer: C
14. Primary syphilitic lesion is called:
A. Gumma
B. Ulcer
C. Chancre
D. Papule
✅ Answer: C
15. Chancre of syphilis is typically:
A. Painful
B. Pus-forming
C. Painless and indurated
D. Necrotic
✅ Answer: C
16. Rash involving palms and soles is seen in:
A. Primary syphilis
B. Secondary syphilis
C. Latent syphilis
D. Tertiary syphilis
✅ Answer: B
17. Condylomata lata occur in:
A. Primary syphilis
B. Secondary syphilis
C. Latent syphilis
D. Congenital syphilis
✅ Answer: B
18. Latent syphilis is characterized by:
A. Severe symptoms
B. Asymptomatic phase
C. CNS involvement
D. Skin gummas
✅ Answer: B
19. Gumma formation occurs in:
A. Primary syphilis
B. Secondary syphilis
C. Latent syphilis
D. Tertiary syphilis
✅ Answer: D
20. Obliterative endarteritis is characteristic of:
A. Tuberculosis
B. Syphilis
C. Leprosy
D. Gonorrhea
✅ Answer: B
21. Non-venereal treponemal disease causing yaws:
A. T. pallidum
B. T. carateum
C. T. pertenue
D. T. denticola
✅ Answer: C
22. Pinta is caused by:
A. T. pallidum
B. T. pertenue
C. T. carateum
D. Borrelia
✅ Answer: C
23. Screening test for syphilis:
A. TPHA
B. FTA-ABS
C. VDRL
D. ELISA only
✅ Answer: C
24. VDRL test detects:
A. Treponemal antibodies
B. Reagin antibodies
C. IgE antibodies
D. Complement proteins
✅ Answer: B
25. Confirmatory test for syphilis:
A. RPR
B. VDRL
C. TPHA
D. ESR
✅ Answer: C
26. Treponemal tests usually remain positive:
A. Only in early disease
B. Until treatment
C. For life
D. For 6 months
✅ Answer: C
27. Best test to monitor treatment response:
A. TPHA
B. FTA-ABS
C. VDRL titer
D. ELISA
✅ Answer: C
28. CSF-VDRL is used to diagnose:
A. Congenital syphilis
B. Primary syphilis
C. Neurosyphilis
D. Latent syphilis
✅ Answer: C
29. Drug of choice for syphilis:
A. Azithromycin
B. Ciprofloxacin
C. Penicillin G
D. Doxycycline
✅ Answer: C
30. Resistance to penicillin in T. pallidum is:
A. Common
B. Increasing
C. Rare but present
D. Not documented
✅ Answer: D
31. Macrolide resistance in T. pallidum is due to mutation in:
A. gyrA gene
B. 16S rRNA
C. 23S rRNA
D. rpoB
✅ Answer: C
32. Alternative drug in penicillin allergy:
A. Metronidazole
B. Doxycycline
C. Amikacin
D. Vancomycin
✅ Answer: B
33. Congenital syphilis occurs due to:
A. Breastfeeding
B. Sexual contact
C. Transplacental transmission
D. Blood transfusion
✅ Answer: C
34. Hutchinson teeth are seen in:
A. Primary syphilis
B. Secondary syphilis
C. Congenital syphilis
D. Latent syphilis
✅ Answer: C
35. Treponema pallidum lacks:
A. Cell wall
B. Capsule
C. Axial filaments
D. Outer membrane
✅ Answer: B
36. Antigenic variation in T. pallidum helps in:
A. Rapid multiplication
B. Immune evasion
C. Antibiotic resistance
D. Sporulation
✅ Answer: B
37. Best prevention of syphilis:
A. Vaccination
B. Antibiotic prophylaxis
C. Safe sexual practices
D. Isolation
✅ Answer: C
38. Vaccine for syphilis is:
A. Available
B. Under trial
C. Partially effective
D. Not available
✅ Answer: D
39. Antenatal screening prevents:
A. Secondary syphilis
B. Neurosyphilis
C. Congenital syphilis
D. Tertiary syphilis
✅ Answer: C
40. Treponema pallidum outer membrane has:
A. Many exposed proteins
B. Lipopolysaccharide
C. Few exposed antigens
D. Thick capsule
✅ Answer: C
41. Dark-field microscopy is NOT useful in:
A. Genital chancre
B. Oral lesions
C. Secondary syphilis
D. Early syphilis
✅ Answer: B
42. Which test may give false-positive results?
A. TPHA
B. FTA-ABS
C. VDRL
D. PCR
✅ Answer: C
43. Mode of transmission of yaws:
A. Sexual
B. Vector-borne
C. Direct skin contact
D. Airborne
✅ Answer: C
44. Pinta mainly affects:
A. CNS
B. Cardiovascular system
C. Skin
D. Bone marrow
✅ Answer: C
45. Treponema pallidum survives poorly outside host due to:
A. Capsule
B. Spores
C. Fragile nature
D. Acid resistance
✅ Answer: C
46. Shape of Treponema pallidum is:
A. Curved comma
B. Straight rod
C. Tight spiral
D. Oval cocci
✅ Answer: C
47. Treponema pallidum energy source is mainly:
A. Fatty acids
B. Host-derived glucose
C. Amino acid fermentation
D. Nitrate reduction
✅ Answer: B
48. Non-treponemal tests detect antibodies against:
A. Flagella
B. Cardiolipin
C. DNA
D. Protein antigens
✅ Answer: B
49. Which stage is most infectious?
A. Latent
B. Tertiary
C. Primary & Secondary
D. Congenital
✅ Answer: C
50. Best public health measure to control syphilis:
A. Mass vaccination
B. Early diagnosis and treatment
C. Vector control
D. Isolation only
✅ Answer: B