Introduction
- Giardia lamblia (also known as Giardia intestinalis or Giardia duodenalis) is a protozoan parasite and one of the most common causes of intestinal infections worldwide.
- It belongs to the class Zoomastigophorea and is responsible for giardiasis, a diarrheal disease that significantly affects humans and various animals.
- The parasite alternates between two forms: the motile trophozoite and the environmentally resistant cyst, facilitating survival and transmission.
- Giardiasis is prevalent in regions with poor sanitation but can also affect individuals in developed countries, especially hikers, travelers, or those exposed to untreated water.
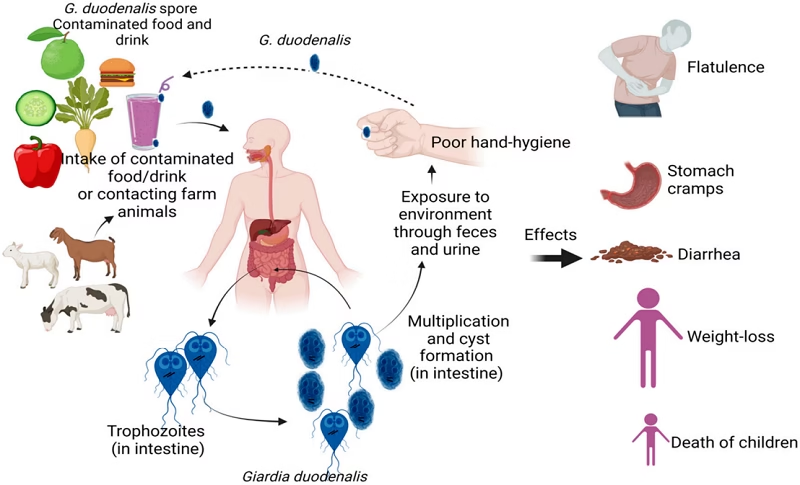
- The disease is transmitted via the fecal-oral route, often through contaminated food, water, or person-to-person contact.
- Symptoms range from mild gastrointestinal discomfort to severe malabsorption and chronic diarrhea.
- Understanding Giardia’s biology and life cycle is crucial for effective diagnosis, treatment, and prevention.
Geographical Distribution
Giardia lamblia has a global distribution, affecting people across all continents.
- Endemic regions: The highest prevalence occurs in low-income countries with inadequate sanitation, including parts of Africa, Asia, Latin America, and Eastern Europe.
- Developed regions: In industrialized countries, outbreaks are often associated with contaminated water sources or food, especially during recreational activities (e.g., swimming in lakes or rivers).
- High-risk populations: Children in daycare centers, immunocompromised individuals, travelers, hikers, and refugees are particularly vulnerable.
Habitat
The habitat of Giardia lamblia varies based on its life cycle stage:
- Trophozoite:
- Resides in the small intestine, particularly the duodenum and jejunum.
- Attaches to intestinal epithelial cells using a ventral adhesive disc but does not invade tissue.
- Thrives in an anaerobic or microaerophilic environment.
- Cyst:
- Found in the colon during the encystation phase and excreted in feces.
- Survives in external environments, including water, soil, and food, for weeks to months due to its tough, protective wall.
Morphology
Giardia lamblia exhibits two distinct morphological forms:
Trophozoite:
-
- Shape: Pear-shaped (teardrop-like).
- Size: 9–21 µm in length and 5–15 µm in width.
- Structure:
- Binucleate, with two prominent nuclei containing central karyosomes.
- Ventral adhesive disc for attachment to the intestinal mucosa.
- Four pairs of flagella (8 total) for motility.
- Function: Active feeding and reproduction stage in the host’s intestine.
Cyst:
-
- Shape: Oval.
- Size: 8–14 µm in length and 7–10 µm in width.
- Structure:
- Protective thick wall, enabling survival in harsh conditions.
- Four nuclei (mature cyst).
- Internally contains retracted flagella and trophozoite precursors.
- Function: Infective stage; facilitates transmission between hosts.
Life Cycle
The life cycle of Giardia lamblia involves two stages and is completed in a single host:
- Ingestion:
- Infection begins when cysts are ingested via contaminated water, food, or direct contact.
- Excystation:
- In the stomach and duodenum, gastric acid and intestinal enzymes trigger the release of trophozoites from cysts.
- Each cyst produces two trophozoites.
- Colonization:
- Trophozoites multiply asexually (binary fission) and attach to the intestinal epithelium.
- This leads to disruption of intestinal functions.
- Encystation:
- In the colon, trophozoites encyst under unfavorable conditions (e.g., dehydration).
- Excretion:
- Cysts are passed in feces, surviving in the environment until a new host ingests them.
Mode of Transmission
Giardia lamblia is transmitted via the fecal-oral route:
- Waterborne transmission:
- Drinking or recreational water contaminated with cysts is the most common mode.
- Outbreaks often occur in settings with untreated or poorly treated water supplies.
- Foodborne transmission:
- Consumption of food contaminated by infected handlers or exposure to untreated irrigation water.
- Person-to-person transmission:
- Common in daycare centers, nursing homes, and households due to poor hygiene.
- It can also occur through oral-anal contact, particularly in sexual practices.
- Zoonotic transmission:
- Cysts from infected animals (e.g., beavers, dogs, livestock) can contaminate water sources.
Incubation Time
The incubation period for giardiasis ranges from 1 to 2 weeks (commonly 7–10 days) after the ingestion of cysts. This variability depends on the infective dose, host immune status and other environmental factors.
Pathogenesis
The pathogenic mechanisms of Giardia lamblia involve both mechanical and biochemical effects:
- Adhesion to the intestinal mucosa:
- Trophozoites attach to epithelial cells using their ventral adhesive discs.
- This causes mechanical irritation and damage to the intestinal lining.
- Disruption of absorption:
- Villous atrophy and crypt hyperplasia reduce the absorptive surface area of the small intestine.
- Leads to the malabsorption of nutrients, particularly fats, carbohydrates, and vitamins (e.g., vitamin B12).
- Enzymatic dysfunction:
- Decreased activity of brush border enzymes (e.g., lactase) causes lactose intolerance and osmotic diarrhea.
- Immune response:
- The host’s immune response to the parasite can lead to inflammation, further exacerbating diarrhea and nutrient loss.
Clinical Manifestations
1. Asymptomatic Infection
Many infected individuals do not develop symptoms and act as carriers of the parasite.
Features
- No apparent symptoms
- Cysts are passed in stool
- Serve as a source of infection for others
2. Acute Giardiasis
Symptoms usually appear 1–3 weeks after ingestion of cysts.
Gastrointestinal Symptoms
Diarrhea
- Most common symptom
- Usually watery and foul-smelling
- May occur several times a day
Abdominal Cramps
- Cramping pain around the abdomen
- Often associated with diarrhea
Bloating and Abdominal Distension
- Feeling of fullness
- Increased gas formation
Flatulence
- Excessive passage of gas
- Common complaint in giardiasis
Nausea and Vomiting
- Mild to moderate nausea
- Vomiting may occur occasionally
Loss of Appetite
- Reduced desire to eat
- May contribute to weight loss
3. Chronic Giardiasis
If the infection persists for weeks or months, chronic symptoms may develop.
Persistent Diarrhea
- Recurrent episodes of loose stools
- May alternate with normal bowel movements
Weight Loss
- Due to poor absorption of nutrients
- Common in prolonged infections
Fatigue and Weakness
- Result from malnutrition and dehydration
Malabsorption Syndrome
- Impaired absorption of nutrients from the intestine
- One of the most important complications
4. Steatorrhea (Fatty Stool)
A characteristic feature of chronic giardiasis.
Features
- Pale, bulky stools
- Greasy appearance
- Foul odor
- Difficult to flush
Cause
- Impaired fat absorption in the small intestine
5. Nutritional Deficiencies
Long-standing infection may lead to deficiency of:
- Fat-soluble vitamins (A, D, E, K)
- Vitamin B12
- Folic acid
- Iron
Consequences
- Weakness
- Poor growth
- Anemia
6. Lactose Intolerance
Giardia may damage intestinal villi and reduce lactase enzyme activity.
Symptoms
- Bloating after consuming milk
- Abdominal discomfort
- Increased diarrhea
7. Clinical Manifestations in Children
Children are more severely affected because of their increased nutritional requirements.
Features
- Chronic diarrhea
- Growth retardation
- Weight loss
- Malnutrition
- Poor school performance
- Delayed physical development
8. Clinical Manifestations in Immunocompromised Patients
In patients with weakened immunity, symptoms may be more severe and prolonged.
Features
- Persistent diarrhea
- Severe malabsorption
- Marked weight loss
- Recurrent infection
Laboratory Diagnosis
Accurate diagnosis of giardiasis involves the detection of Giardia lamblia in stool or intestinal samples:
1. Stool Microscopic Examination
- Stool examination is the most common and widely used method for diagnosing giardiasis.
Specimen Collection
- Fresh stool sample is preferred.
- Multiple stool samples (usually three samples collected on alternate days) should be examined because cyst excretion is intermittent.
- Stool should be examined immediately if trophozoites are suspected.
Findings
Trophozoites
Usually seen in:
- Fresh diarrheal stool
Characteristics:
- Pear-shaped
- Bilaterally symmetrical
- Two nuclei
- Four pairs of flagella
- Characteristic “falling leaf” motility
Cysts
Usually seen in:
- Formed or semi-formed stool
Characteristics:
- Oval-shaped
- Thick-walled
- Mature cyst contains four nuclei
2. Direct Wet Mount Examination
Saline Wet Mount
Used to detect:
- Motile trophozoites
- Cysts
Advantages:
- Simple
- Rapid
- Inexpensive
Iodine Wet Mount
Used to demonstrate:
- Internal structures of cysts
- Nuclei and axonemes
Iodine kills trophozoites but provides better visualization of cyst morphology.
3. Concentration Techniques
When parasites are present in small numbers, concentration methods improve detection.
Formalin-Ether Sedimentation Technique
- Most commonly used concentration method.
- Concentrates cysts and trophozoites.
Zinc Sulfate Flotation Technique
- Useful for detecting Giardia cysts.
- Provides cleaner preparations for microscopic examination.
Advantages
- Increases sensitivity.
- Helpful in chronic infections with low parasite load.
4. Permanent Stained Smears
Permanent staining helps confirm the diagnosis and study parasite morphology.
Common Stains
Trichrome Stain
- Most commonly used stain.
- Demonstrates nuclei and internal structures clearly.
Iron Hematoxylin Stain
- Provides excellent morphological detail.
- Useful for research and reference laboratories.
5. Duodenal Aspirate Examination
Since Giardia inhabits the upper small intestine, trophozoites can sometimes be detected directly from duodenal contents.
Procedure
- Duodenal fluid is collected through intubation.
- Microscopic examination is performed.
Advantages
- Useful when stool examinations are repeatedly negative.
6. Entero-Test (String Test)
This test is used to collect duodenal secretions without intubation.
Procedure
- The patient swallows a gelatin capsule attached to a nylon string.
- After several hours, the string is withdrawn.
- Duodenal mucus adhering to the string is examined microscopically.
Advantages
- Less invasive than duodenal aspiration.
- Useful in difficult diagnostic cases.
7. Antigen Detection Tests
These tests detect Giardia-specific antigens in stool.
Methods
ELISA (Enzyme-Linked Immunosorbent Assay)
- Highly sensitive
- Highly specific
Rapid Immunochromatographic Tests
- Quick results
- Easy to perform
Advantages
- Detect infection even when cysts are not visible.
- Useful in screening large numbers of samples.
8. Molecular Methods
Polymerase Chain Reaction (PCR)
PCR detects Giardia DNA in stool specimens.
Advantages
- Very high sensitivity
- Very high specificity
- Can identify different Giardia genotypes
Limitations
- Expensive
- Requires specialized laboratory facilities
9. Histopathological Examination
Rarely required.
Findings
- Trophozoites attached to intestinal mucosa
- Villous atrophy
- Inflammatory changes
Usually performed when intestinal biopsy is done for other reasons.
Summary of Laboratory Diagnosis
| Test | Purpose |
|---|---|
| Stool Microscopy | Detection of trophozoites and cysts |
| Saline Wet Mount | Demonstration of motile trophozoites |
| Iodine Mount | Identification of cyst morphology |
| Concentration Techniques | Increase parasite recovery |
| Trichrome Stain | Detailed morphology |
| Duodenal Aspirate | Direct detection of trophozoites |
| Entero-Test | Collection of duodenal secretions |
| ELISA | Detection of Giardia antigen |
| Rapid Antigen Tests | Quick diagnosis |
| PCR | Detection of Giardia DNA |
Treatment
Giardiasis treatment aims to eliminate the parasite, resolve symptoms, and prevent transmission.
- Antiparasitic Drugs:
- Metronidazole: First-line treatment (250 mg three times daily for 5–7 days in adults).
- Tinidazole: Single-dose therapy (2 g).
- Nitazoxanide: An effective alternative for children and adults.
- Albendazole: Occasionally used, particularly in cases of resistance or intolerance to other drugs.
- Supportive Therapy:
- Oral rehydration solutions to manage dehydration caused by diarrhea.
- Nutritional support to address malabsorption.
- Treatment of Asymptomatic Carriers:
- Recommended in high-risk settings to prevent transmission (e.g., daycare centers).
- Prevention of Resistance:
- Avoid overuse of antiparasitic drugs; follow proper dosing regimens.
Prevention and Control
Preventing giardiasis requires a combination of personal hygiene, sanitation, and environmental interventions:
- Hygiene practices:
- Handwashing with soap, especially after using the toilet and before eating.
- Water safety:
- Boil or filter drinking water, especially in endemic areas or during outdoor activities.
- Food safety:
- Wash raw fruits and vegetables thoroughly.
- Public health measures:
- Improved sanitation and wastewater management.
- Education campaigns to raise awareness about giardiasis transmission.