Introduction
- Candida is a genus of yeast-like fungi that is commonly found in the human microbiota, particularly in the mucous membranes of the mouth, skin, gastrointestinal tract, and vagina.
- While Candida species are typically harmless in healthy individuals, they can become pathogenic under certain conditions, leading to various infections known as candidiasis.
- Candidiasis can range from superficial infections, such as oral thrush and vaginal yeast infections, to more severe systemic infections, particularly in immunocompromised individuals.
- The most common species associated with human infections is Candida albicans, but other species, such as Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei, are also of clinical significance.
- Diagnosing Candida infections requires careful laboratory techniques, as the manifestations can be nonspecific, and treatment depends on the species involved, the site of infection, and the patient’s health status.
Etiology
The genus Candida comprises over 150 species, but only a few are commonly associated with human infections. The primary etiologic agents of candidiasis are:
- Candida albicans: The most prevalent and pathogenic species responsible for a wide range of infections, from superficial to systemic.
- Candida glabrata: Known for its resistance to azoles, a common class of antifungal drugs.
- Candida tropicalis: Frequently associated with infections in immunocompromised patients, especially those with hematologic malignancies or undergoing organ transplants.
- Candida parapsilosis: Often associated with healthcare-associated infections, particularly in neonates or patients with implanted medical devices.
- Candida krusei: Notably resistant to fluconazole, making infections difficult to treat.
Specimens
Candida infections can be diagnosed from various clinical specimens depending on the infection site. Common specimens include:
- Swabs from affected mucosal areas such as the mouth (oral thrush), skin lesions, or vaginal discharge.
- Blood cultures are used for detecting systemic infections, particularly in immunocompromised patients.
- Urine may be collected for suspected urinary tract infections, especially in patients with indwelling catheters.
- Tissue biopsies from infected sites may be necessary in more severe cases, such as deep or invasive candidiasis.
- Sputum or bronchoalveolar lavage (BAL) samples are used when Candida infection of the lungs is suspected, especially in ventilated patients.
Direct Microscopic Examination
Direct microscopic examination is a critical first step in diagnosing Candida infections. Various methods can be employed, including:
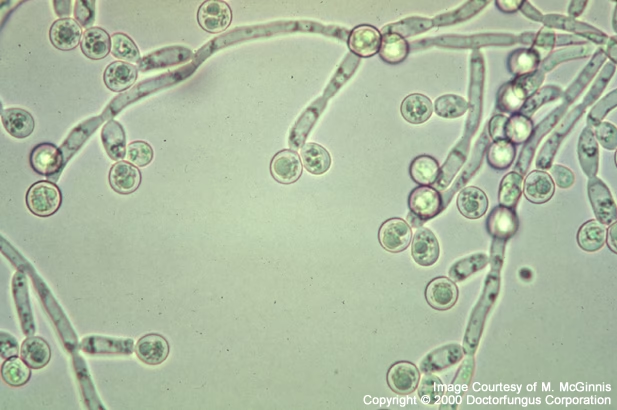
- KOH Mount: A potassium hydroxide (KOH) preparation dissolves the keratin in skin scrapings, allowing for better visualization of fungal elements. Candida appear as budding yeast cells, pseudohyphae, or true hyphae, depending on the growth form.
- Gram Stain: On Gram stain, Candida typically appears as round to oval budding yeast cells, with occasional pseudohyphal forms, especially in clinical samples from the respiratory or gastrointestinal tract.
- India Ink Staining: This method is commonly used for detecting Cryptococcus species in cerebrospinal fluid (CSF), though it is less frequently used for Candida.
- Wet Mount: A saline wet mount can identify Candida yeast and pseudohyphal forms under a microscope for mucosal infections, such as oral thrush.
- Periodic Acid-Schiff (PAS) Staining: PAS staining highlights the fungal cell wall, showing the characteristic cell wall structures of Candida species in tissue specimens.
Culture and Identification
Culturing Candida species is vital for definitive identification and antimicrobial susceptibility testing. Common culture media include:
- Sabouraud Dextrose Agar (SDA): A selective medium that supports fungal growth while inhibiting bacterial growth. Candida species typically form creamy, white colonies on SDA after 24-48 hours of incubation.
- Chromogenic Agar: This specialized medium contains different substrates that, when metabolized by specific Candida species, produce colored colonies. For example, C. albicans may produce green colonies, while C. glabrata forms pink colonies.
- Blood Agar: Provides nutrients for fungal growth and allows observation of hemolysis patterns. Candida species typically show no hemolysis on blood agar.
- Cornmeal Agar: Used for identifying Candida species based on their ability to form pseudohyphae and chlamydospores, which can be observed under the microscope.
After isolation, species identification is carried out using a variety of methods:
- Microscopic Morphology: The formation of pseudohyphae, true hyphae, or chlamydospores on media like cornmeal agar can aid species identification.
- Biochemical Tests: Commercial systems such as API 20C and VITEK 2 can identify Candida species based on their metabolic properties.
- Molecular Methods: PCR-based assays, DNA sequencing, and ribosomal RNA gene analysis are increasingly used for species identification due to their high sensitivity and specificity.
Other Laboratory Tests
In addition to direct microscopic examination and culture, other laboratory tests may help diagnose and manage Candida infections:
- Antifungal Susceptibility Testing: This is especially important in cases of suspected resistant infections. The most common method is the broth dilution test, which determines antifungal agents’ minimum inhibitory concentration (MIC).
- Serological Tests: Tests for antibodies or antigens associated with Candida infections (such as mannan antigen detection) can be used in systemic candidiasis, although they are not commonly used for routine diagnosis.
- PCR and Molecular Assays: PCR-based tests for Candida DNA in clinical specimens provide rapid and sensitive detection, particularly for systemic infections.
- Beta-D-Glucan Assay: This test detects Candida cell wall components and is useful in diagnosing invasive candidiasis, although it may give false positives in patients with certain medical conditions.
Pathogenesis
The pathogenesis of Candida infections involves the yeast’s ability to transition from a harmless commensal organism to a pathogenic one. Host factors, such as immunocompromised states or alterations in the normal microbiota, often trigger this shift. Key factors contributing to the pathogenicity of Candida include:
- Adherence: The ability of Candida to adhere to host tissues is a key factor in initiating infection. This is mediated by surface proteins such as adhesins.
- Dimorphism: Candida species can switch between a yeast form (unicellular) and a hyphal or pseudohyphal form. The hyphal form is particularly associated with tissue invasion.
- Biofilm Formation: Candida can form biofilms on surfaces like catheters, prosthetic devices, and mucosal tissues, which makes the organism more resistant to antifungal treatment and the host immune system.
- Immune Evasion: Candida has evolved mechanisms to evade the host immune system, such as altering its cell wall to avoid detection and utilizing host-derived nutrients to enhance survival.
- Toxin Production: Certain Candida species produce toxins that contribute to tissue damage and facilitate the spread of infection.
Treatment of Candida Infections
Treatment of Candida infections depends on the site of infection, the species involved, and the patient’s immune status. Options include:
- Topical Antifungals: For superficial infections, such as oral thrush, vulvovaginal candidiasis, or cutaneous candidiasis, topical antifungal creams, ointments, or lozenges are often sufficient. Common agents include:
- Clotrimazole
- Miconazole
- Nystatin
- Systemic Antifungals: Antifungal therapy is required for more severe or invasive infections. The most commonly used systemic antifungals include:
- Azoles (e.g., Fluconazole, Itraconazole): These inhibit the synthesis of ergosterol, a key component of the fungal cell membrane.
- Echinocandins (e.g., Caspofungin, Micafungin): These drugs inhibit the synthesis of glucan, an essential component of the fungal cell wall. They are often used for resistant strains of Candida.
- Polyene Antifungals (e.g., Amphotericin B): Often reserved for severe infections or those resistant to azoles, amphotericin B binds to ergosterol in the cell membrane, creating pores that lead to cell death.
- Management of Underlying Conditions: For immunocompromised patients or those with underlying conditions (e.g., diabetes, HIV/AIDS), managing the underlying disease is crucial in controlling Candida infections. This may involve the use of immunosuppressive drugs or glucose control.
- Prophylactic Antifungal Therapy: In high-risk patients, such as those undergoing chemotherapy or organ transplantation, prophylactic antifungal treatment may be administered to prevent Candida infections.