Introduction
- Entamoeba gingivalis is a unicellular protozoan parasite that inhabits the human oral cavity.
- It is one of the most common amoebae found in humans and is primarily located in gingival crevices, periodontal pockets, dental plaque, and tonsillar crypts.
- Unlike many parasitic amoebae, Entamoeba gingivalis does not possess a cyst stage and exists exclusively in the trophozoite form.
- The organism was first described by Gros in 1849 and is considered the first amoeba identified in humans.
- For many years, it was regarded as a harmless commensal organism.
- However, recent studies have suggested a possible association between Entamoeba gingivalis and periodontal diseases such as gingivitis and chronic periodontitis.
Geographical Distribution
Entamoeba gingivalis is found worldwide, with no specific geographical restrictions. Its prevalence varies depending on oral hygiene practices, age, and the presence of periodontal disease.
- Higher prevalence:
- Individuals with poor oral hygiene.
- Patients with periodontal disease, gingivitis, or other oral infections.
- Lower prevalence:
- Populations with good dental care and oral hygiene practices.
Habitat
E. gingivalis primarily resides in the oral cavity, particularly in the:
- Gingival crevices.
- Periodontal pockets.
- Tonsillar crypts.
- Dental plaques.
The parasite feeds on epithelial cells, bacteria, leukocytes, and other debris found in these regions, especially in areas with active inflammation or infection.
Morphology
Trophozoite
The trophozoite is the only developmental stage present in Entamoeba gingivalis.
Size
The trophozoites typically measure between 10 and 35 μm in diameter, although larger forms may occasionally be observed.
Shape
The organism exhibits an irregular shape due to the continuous formation of pseudopodia. These cytoplasmic extensions facilitate locomotion and feeding.
Cytoplasm
The cytoplasm is differentiated into:
Ectoplasm
The clear outer layer responsible for pseudopod formation and movement.
Endoplasm
The granular inner layer containing various cellular organelles and ingested materials.
Nucleus
The nucleus is usually spherical and contains:
- Thin nuclear membrane
- Fine peripheral chromatin
- Small central karyosome
The nucleus may be difficult to visualize in unstained preparations.
Food Vacuoles
Numerous food vacuoles are commonly present and may contain:
- Bacteria
- Leukocytes
- Epithelial cells
- Cellular debris
One characteristic feature of Entamoeba gingivalis is its ability to ingest leukocytes, a process known as leukophagocytosis.
Life Cycle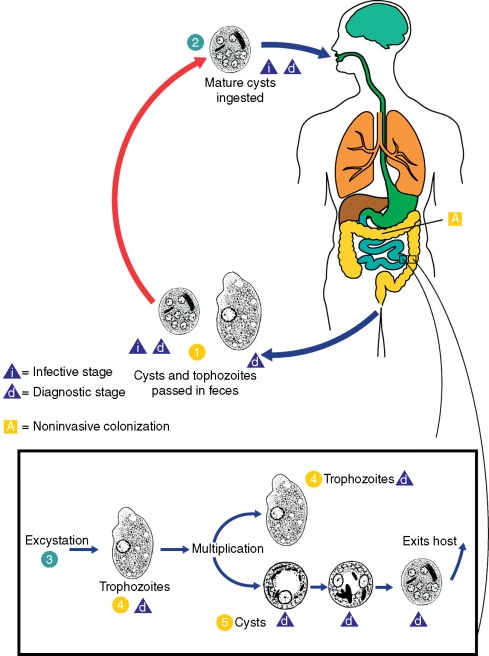
The life cycle of E. gingivalis is simple and involves only the trophozoite stage.
Entamoeba gingivalis possesses a simple direct life cycle.
Absence of Cyst Stage
Unlike Entamoeba histolytica and several other intestinal amoebae, Entamoeba gingivalis does not form cysts. Consequently, transmission requires direct transfer of trophozoites between individuals.
Reproduction
The parasite reproduces asexually through binary fission.
During this process:
- Nuclear division occurs.
- Cytoplasmic division follows.
- Two daughter trophozoites are produced.
Transmission
Transmission occurs through direct exchange of saliva.
Common routes include:
- Kissing
- Sharing eating utensils
- Sharing drinking glasses
- Sharing toothbrushes
- Close personal contact
After entering a new host, trophozoites colonize gingival tissues and multiply locally.
Epidemiology
The prevalence of Entamoeba gingivalis varies according to age, oral hygiene status, and periodontal health.
Healthy Individuals: Reported prevalence ranges from 5–30%.
Gingivitis Patients: Prevalence may increase to 40–70%.
Chronic Periodontitis Patients: Several studies report prevalence rates exceeding 80%.
Risk Factors
Important risk factors include:
- Poor oral hygiene
- Dental plaque accumulation
- Smoking
- Diabetes mellitus
- Immunosuppression
- Advanced age
- Malnutrition
- Chronic inflammatory conditions
Pathogenesis
The pathogenicity of Entamoeba gingivalis remains an area of active investigation.
Several mechanisms have been proposed.
Leukophagocytosis
The organism actively ingests leukocytes, particularly neutrophils.
This may:
- Impair local immune defenses
- Prolong inflammatory responses
- Facilitate microbial survival
Tissue Irritation
Movement of trophozoites within gingival tissues may contribute to:
- Local irritation
- Chronic inflammation
- Tissue damage
Synergistic Interaction with Bacteria
Periodontal disease is primarily caused by bacterial biofilms. Entamoeba gingivalis may interact with periodontal pathogens, enhancing tissue destruction.
Common associated bacteria include:
- Porphyromonas gingivalis
- Tannerella forsythia
- Treponema denticola
Inflammatory Response
The parasite may stimulate the production of inflammatory mediators, leading to:
- Gingival swelling
- Increased vascular permeability
- Connective tissue destruction
Clinical Manifestations
Most infected individuals remain asymptomatic.
Clinical manifestations are generally associated with concurrent periodontal disease.
Gingivitis
Features include:
- Red swollen gums
- Bleeding during brushing
- Mild discomfort
- Plaque accumulation
Periodontitis
Advanced disease may present with:
- Deep periodontal pockets
- Gum recession
- Bone loss
- Tooth mobility
- Tooth loss
Halitosis
Persistent bad breath may occur due to heavy microbial colonization
Mode of Transmission
- gingivalis is transmitted primarily through:
- Saliva exchange:
- Kissing or sharing utensils, toothbrushes, or other oral items.
- Contact with oral secretions:
- Close personal contact or indirect transmission through contaminated dental instruments.
- Association with dental procedures:
- Invasive dental treatments may facilitate its spread.
Unlike E. histolytica, E. gingivalis is not transmitted through the fecal-oral route since it lacks a cyst stage.
Incubation Time
- There is no defined incubation period for E. gingivalis as it is not always pathogenic.
- Its presence in the oral cavity may persist for extended periods without causing noticeable symptoms unless oral hygiene deteriorates or periodontal disease develops.
Laboratory Diagnosis
Specimen Collection
Appropriate specimen collection is essential for accurate diagnosis. Samples are usually obtained from sites where the organism is most abundant.
Common Specimens
- Gingival scrapings
- Dental plaque
- Periodontal pocket exudates
- Gingival crevice material
- Tonsillar crypt debris
- Oral swabs from inflamed gingival areas
Samples should be transported and examined immediately because trophozoites rapidly lose motility outside the host.
Direct Wet Mount Examination
Direct microscopy remains the simplest and most widely used method for detecting Entamoeba gingivalis.
Procedure
- Place a small amount of freshly collected plaque or gingival material on a clean glass slide.
- Add a drop of normal saline.
- Cover with a coverslip.
- Examine under low-power (10×) and high-power (40×) objectives.
Microscopic Findings
Characteristic findings include:
- Actively motile trophozoites
- Amoeboid movement
- Formation of pseudopodia
- Granular cytoplasm
- Presence of food vacuoles
- Ingested bacteria
- Ingested leukocytes (leukophagocytosis)
The observation of active pseudopodial movement is one of the most important diagnostic features.
Advantages
- Rapid diagnosis
- Inexpensive
- Simple technique
- No specialized equipment required
Limitations
- Requires fresh specimens
- Lower sensitivity in light infections
- Operator-dependent interpretation
Stained Smear Examination
Permanent stained preparations provide better visualization of cellular structures and aid in definitive identification.
Giemsa Staining
Giemsa stain is commonly used for demonstrating protozoal morphology.
Findings
- Distinct nucleus
- Small central karyosome
- Fine peripheral chromatin
- Cytoplasmic vacuoles
- Ingested cellular debris
Wheatley’s Trichrome Stain
Trichrome staining improves contrast and facilitates differentiation from other cellular elements.
Findings
- Well-defined cytoplasm
- Clear nuclear morphology
- Enhanced visualization of trophozoite structure
Hematoxylin Staining
Iron hematoxylin stain may be used to demonstrate nuclear details more clearly.
Advantages of Stained Smears
- Better morphological preservation
- Permanent record for documentation
- Improved identification accuracy
Phase-Contrast Microscopy
Phase-contrast microscopy allows visualization of living trophozoites without staining.
Advantages
- Enhanced observation of motility
- Better visualization of pseudopodia
- Useful for fresh specimens
This technique is particularly valuable when studying trophozoite behavior and movement.
Culture Methods
Cultivation of Entamoeba gingivalis is rarely performed in routine laboratories but may be useful for research purposes.
Culture Media
Specialized media containing:
- Serum
- Bacterial flora
- Nutrient supplements
can support trophozoite growth.
Limitations
- Time-consuming
- Technically demanding
- Not routinely used for clinical diagnosis
Molecular Diagnosis
Molecular techniques have become increasingly important due to their high sensitivity and specificity.
Polymerase Chain Reaction (PCR)
PCR is currently considered the most sensitive method for detecting Entamoeba gingivalis.
Principle
PCR amplifies species-specific DNA sequences present in oral samples.
Advantages
- High sensitivity
- High specificity
- Detection of low parasite loads
- Useful in asymptomatic infections
- Identification of genetic variants
Applications
- Epidemiological studies
- Research investigations
- Confirmation of microscopic findings
PCR studies have shown that infection rates may be significantly higher than those detected by conventional microscopy.
Real-Time PCR
Real-time PCR offers several advantages over conventional PCR.
Benefits
- Rapid detection
- Quantification of parasite DNA
- Reduced contamination risk
- High diagnostic accuracy
This method is increasingly used in research laboratories investigating periodontal diseases.
DNA Sequencing
DNA sequencing techniques are used mainly for research purposes.
Applications
- Identification of genetic subtypes
- Study of strain diversity
- Evolutionary analysis
- Investigation of pathogenic mechanisms
Recent studies have revealed genetic heterogeneity among Entamoeba gingivalis isolates.
Differential Diagnosis
During microscopic examination, Entamoeba gingivalis must be distinguished from several other structures.
Macrophages
Macrophages may resemble amoebae but lack active pseudopodial movement.
Neutrophils
Neutrophils are smaller and possess multilobed nuclei.
Oral Epithelial Cells
These cells are larger, non-motile, and have distinct cellular boundaries.
Entamoeba histolytica
Although morphologically similar, E. histolytica primarily inhabits the intestine and produces cysts, whereas E. gingivalis does not.
Diagnostic Criteria
A diagnosis of Entamoeba gingivalis is generally established by demonstrating:
- Motile trophozoites in fresh oral specimens
- Characteristic pseudopodia
- Single nucleus with central karyosome
- Cytoplasmic food vacuoles
- Presence of ingested leukocytes or bacteria
Confirmation may be obtained using PCR-based methods when available.
Laboratory Diagnostic Methods
| Method | Utility | Sensitivity |
|---|---|---|
| Direct Wet Mount | Routine diagnosis | Moderate |
| Giemsa Stain | Morphological identification | Moderate |
| Trichrome Stain | Detailed morphology | Moderate |
| Phase-Contrast Microscopy | Motility studies | Moderate |
| Culture | Research purposes | Low |
| Conventional PCR | Species confirmation | High |
| Real-Time PCR | Quantitative detection | Very High |
| DNA Sequencing | Genetic analysis | Very High |
Treatment
Treatment of E. gingivalis infections focuses on eliminating the parasite and addressing underlying oral conditions, such as periodontal disease.
Antiparasitic Therapy:
- Metronidazole: Effective against E. gingivalis trophozoites. Typically prescribed in combination with dental treatments.
- Chlorhexidine mouthwash: Reduces microbial load and may help control parasite numbers.
Dental Care:
- Professional dental cleaning to remove plaques and calculus.
- Periodontal therapy for patients with gum disease.
Oral Hygiene:
- Regular brushing, flossing, and use of antiseptic mouthwashes to maintain a healthy oral environment and prevent recolonization.
Prevention
Maintain Good Oral Hygiene:
- Brush and floss regularly to minimize plaque buildup.
Avoid Sharing Oral Items:
- Avoid sharing utensils, toothbrushes, or dental appliances.
Regular Dental Checkups:
- Routine professional cleaning and assessment can reduce the risk of colonization.
Sterilisation of Dental Instruments:
- Proper sterilization practices in dental clinics prevent cross-contamination.