Introduction
-
Klebsiella pneumoniae is a Gram-negative, non-motile, encapsulated bacillus
-
It belongs to the family Enterobacteriaceae
-
It is a facultative anaerobe
-
Normally present as a commensal in the human gastrointestinal tract
-
Acts as an opportunistic pathogen, especially in hospitalized and immunocompromised patients
-
Characterized by a thick polysaccharide capsule, which is a major virulence factor
-
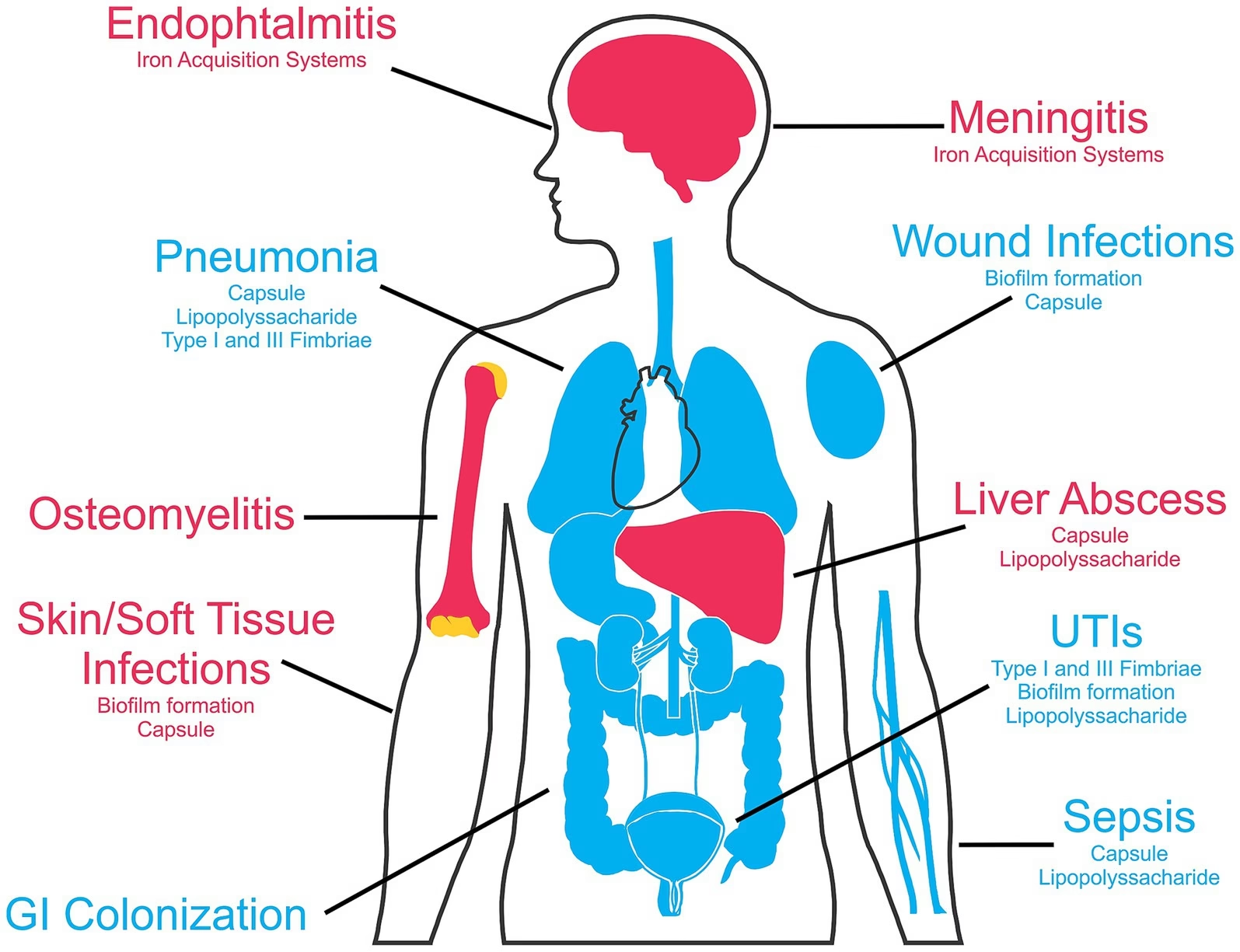
Commonly causes pneumonia, urinary tract infections, septicemia, and wound infections
-
Produces mucoid colonies on culture media due to capsule production
-
Increasingly important due to multidrug resistance, including ESBL and carbapenemase production
-
A significant cause of nosocomial infections worldwide
General Character
Genus: Klebsiella
Species: Klebsiella pneumoniae
Family: Enterobacteriaceae
Gram Staining
Klebsiella pneumoniae is a Gram-negative bacterium.
On Gram staining, it appears pink due to the presence of a thin peptidoglycan layer and an outer lipopolysaccharide membrane.
Shape and Arrangement
- Shape: Rod-shaped (bacilli)
- Arrangement: Commonly seen as single cells; may occasionally form short chains
Oxygen Requirement
Klebsiella species are facultative anaerobes, meaning they can grow in both aerobic and anaerobic environments.
Morphology
-
Shape: Short, plump rod-shaped bacilli
-
Size: Approximately 1–2 µm in length and 0.5–0.8 µm in width
-
Gram Reaction: Gram-negative
-
Capsule:
-
Possesses a prominent polysaccharide capsule
-
Capsule gives a mucoid appearance to colonies
-
Best demonstrated by negative staining (India ink)
-
Important virulence factor – protects against phagocytosis
-
-
Motility: Non-motile (absence of flagella)
-
Spores: Non-spore forming
-
Arrangement: Occur singly, in pairs, or occasionally in short chains
-
Special Staining Features:
-
Capsule seen as a clear halo around the bacillus in capsule staining
-
Cultural Characteristics
1. Growth on Nutrient Agar
-
Produces large, smooth, convex, glistening colonies
-
Colonies are mucoid and sticky
-
Color: Greyish-white
-
Mucoid nature is due to abundant capsular polysaccharide
2. Growth on Blood Agar
-
Forms large, dome-shaped, mucoid colonies
-
Non-hemolytic (γ-hemolysis)
-
Colonies may show a stringy appearance when touched with a loop
3. Growth on MacConkey Agar
-
Produces large, pink, mucoid colonies
-
Lactose fermenter
-
Pink color due to acid production from lactose fermentation
-
Colonies are often very sticky and glistening
4. Growth in Liquid Media (Nutrient Broth)
-
Causes uniform turbidity
-
May produce a surface pellicle
-
Sometimes forms stringy sediment due to capsule
5. Special Features
-
Colonies show a positive string test (string >5 mm when stretched with loop)
-
Mucoid growth is an important diagnostic clue
6. Temperature and pH
-
Optimum temperature: 37°C
-
Can grow at room temperature
-
Optimum pH: 7.2–7.4
Biochemical Reactions
Catalase Test
-
Positive
-
Produces effervescence (bubbles) when hydrogen peroxide is added
Oxidase Test
-
Negative
-
Helps distinguish Klebsiella from oxidase-positive Gram-negative bacteria (e.g., Pseudomonas)
Lactose Fermentation
-
Positive
-
Ferments lactose with production of acid and gas
-
Produces pink, mucoid colonies on MacConkey agar
Indole Production
-
Negative in Klebsiella pneumoniae
-
Helps differentiate from indole-positive species such as Klebsiella oxytoca
Methyl Red (MR) Test
-
Negative
-
Indicates absence of mixed acid fermentation
Voges–Proskauer (VP) Test
-
Positive
-
Indicates production of acetoin via the butylene glycol pathway
Pathogenicity
Virulence Factors
-
Capsule (K antigen)
-
Thick polysaccharide capsule
-
Inhibits phagocytosis and complement-mediated killing
-
Responsible for mucoid colonies
-
Major determinant of virulence
-
-
Lipopolysaccharide (LPS / Endotoxin)
-
Causes fever, inflammation, shock
-
Contributes to sepsis
-
-
Fimbriae (Pili)
-
Aid in adhesion to respiratory and urinary tract epithelium
-
Important in urinary tract infections
-
-
Siderophores (e.g., Enterobactin)
-
Help in iron acquisition
-
Enhance bacterial survival in host tissues
-
-
Biofilm Formation
-
Promotes persistence on medical devices (catheters, ventilators)
-
Contributes to antibiotic resistance
-
Diseases Caused
-
Pneumonia
-
Classically causes lobar pneumonia
-
Produces thick, blood-tinged “currant jelly” sputum
-
Common in alcoholics, diabetics, elderly
-
-
Urinary Tract Infections (UTI)
-
Common nosocomial pathogen
-
Associated with catheterization
-
-
Septicemia (Bacteremia)
-
Can lead to septic shock
-
High mortality in immunocompromised patients
-
-
Wound and Surgical Site Infections
-
Especially in hospitalized patients
-
-
Liver Abscess
-
Seen particularly with hypervirulent strains
-
More common in diabetics
-
-
Meningitis
-
Rare, but occurs in neonates and immunocompromised adults
-
Mode of Transmission
-
Endogenous flora of gastrointestinal tract
-
Spread via hands of healthcare workers
-
Contaminated hospital equipment
Predisposing Factors
-
Diabetes mellitus
-
Alcoholism
-
Chronic lung disease
-
Prolonged hospital stay
-
Mechanical ventilation
-
Immunosuppression
Laboratory Diagnosis
1. Specimen Collection
Depending on the clinical condition:
-
Sputum – pneumonia
-
Urine – urinary tract infection
-
Blood – septicemia
-
Pus / Wound swab – wound infections
-
CSF – meningitis
2. Direct Microscopy
-
Gram staining of specimen shows:
-
Gram-negative bacilli
-
Often seen singly or in pairs
-
Surrounded by a clear halo due to capsule
-
-
Capsule demonstration:
-
India ink / negative staining
-
Capsule appears as a clear zone around the bacillus
-
3. Culture
-
Nutrient agar: Large, smooth, mucoid colonies
-
Blood agar: Large, mucoid, non-hemolytic colonies
-
MacConkey agar:
-
Large pink mucoid colonies
-
Indicates lactose fermentation
-
-
String test: Positive (string >5 mm)
4. Biochemical Identification
Characteristic reactions include:
-
Lactose fermentation: Positive
-
Indole: Negative
-
Methyl Red: Negative
-
Voges–Proskauer: Positive
-
Citrate utilization: Positive
-
Urease: Positive (weak)
-
Motility: Negative
IMViC pattern: – – + +
5. Automated and Molecular Methods
-
Automated systems: VITEK, MALDI-TOF MS
-
PCR: Detection of virulence genes and resistance genes (e.g., ESBL, carbapenemase genes)
6. Antimicrobial Susceptibility Testing
-
Performed by Kirby–Bauer disk diffusion or MIC determination
-
Important to detect:
-
ESBL-producing strains
-
Carbapenem-resistant Klebsiella pneumoniae (CRKP)
-
7. Serotyping (Specialized Labs)
-
Based on capsular (K) antigens
-
Used mainly for epidemiological studies
Antibiotic Resistance
1. β-Lactamase Production
a. ESBL (Extended-Spectrum β-Lactamases)
-
Hydrolyze:
-
Third-generation cephalosporins (ceftriaxone, ceftazidime)
-
Aztreonam
-
-
ESBL genes: CTX-M, TEM, SHV
-
ESBL producers appear sensitive in vitro but fail clinically
-
Clavulanic acid inhibits ESBL
b. AmpC β-Lactamases
-
Confer resistance to:
-
Cephalosporins
-
Cephamycins
-
-
Not inhibited by clavulanic acid
c. Carbapenemases (CRKP)
-
Hydrolyze carbapenems (imipenem, meropenem)
-
Important enzymes:
-
KPC (Klebsiella pneumoniae carbapenemase)
-
NDM-1 (New Delhi metallo-β-lactamase)
-
OXA-48
-
-
Lead to extensively drug-resistant (XDR) infections
2. Altered Outer Membrane Permeability
-
Loss or mutation of porin proteins
-
Decreases antibiotic entry
-
Commonly associated with carbapenem resistance
3. Efflux Pumps
-
Actively expel antibiotics out of the cell
-
Contribute to resistance against:
-
Fluoroquinolones
-
Tetracyclines
-
4. Target Site Modification
-
Fluoroquinolone resistance due to mutations in:
-
DNA gyrase (gyrA)
-
Topoisomerase IV (parC)
-
5. Plasmid-Mediated Resistance
-
Resistance genes carried on plasmids
-
Enables horizontal gene transfer
-
Leads to rapid spread in hospitals
6. Biofilm-Associated Resistance
-
Biofilm formation on:
-
Catheters
-
Ventilators
-
-
Reduces antibiotic penetration
-
Causes persistent infections
Prevention
1. Hospital Infection Control Measures
-
Strict hand hygiene (alcohol-based hand rubs / soap and water)
-
Use of personal protective equipment (PPE) when indicated
-
Contact precautions for infected or colonized patients
-
Isolation or cohorting of patients with MDR Klebsiella
2. Environmental and Equipment Control
-
Proper sterilization and disinfection of:
-
Ventilators
-
Catheters
-
Endoscopes
-
-
Regular cleaning of hospital surfaces
-
Use of single-use or properly disinfected devices
3. Device-Associated Infection Prevention
-
Aseptic insertion of urinary and intravascular catheters
-
Early removal of catheters and invasive devices
-
Proper care of:
-
Endotracheal tubes
-
Central venous lines
-
4. Antimicrobial Stewardship
-
Rational use of antibiotics
-
Avoid unnecessary:
-
Broad-spectrum antibiotics
-
Prolonged antibiotic therapy
-
-
Regular antibiotic sensitivity testing
-
Hospital antibiotic policy adherence
5. Surveillance and Screening
-
Routine surveillance cultures in high-risk units (ICU, NICU)
-
Early detection of:
-
ESBL-producing strains
-
Carbapenem-resistant Klebsiella pneumoniae
-
-
Prompt outbreak investigation
6. Patient-Related Preventive Measures
-
Good glycemic control in diabetics
-
Nutritional support in debilitated patients
-
Proper management of:
-
Chronic lung disease
-
Alcohol dependence
-
7. Community-Level Prevention
-
Avoid misuse of antibiotics
-
Public awareness about:
-
Antibiotic resistance
-
Hygiene practices
-
8. Vaccination
-
No licensed vaccine currently available against Klebsiella pneumoniae
-
Research ongoing targeting capsular polysaccharides
MCQs
1. Klebsiella pneumoniae belongs to which family?
A. Pseudomonadaceae
B. Enterobacteriaceae
C. Vibrionaceae
D. Neisseriaceae
Answer: B
2. Klebsiella pneumoniae is:
A. Gram-positive cocci
B. Gram-negative bacilli
C. Gram-positive bacilli
D. Gram-negative cocci
Answer: B
3. The arrangement of Klebsiella pneumoniae is usually:
A. Chains
B. Clusters
C. Singles or short chains
D. Diplococci
Answer: C
4. Which structure is the most important virulence factor of Klebsiella?
A. Flagella
B. Capsule
C. Pili
D. Spores
Answer: B
5. Klebsiella pneumoniae is:
A. Motile
B. Spore forming
C. Non-motile
D. Acid-fast
Answer: C
6. On Gram staining, Klebsiella appears:
A. Purple cocci
B. Pink rods
C. Blue spirals
D. Red cocci
Answer: B
7. Klebsiella pneumoniae is best described as:
A. Obligate aerobe
B. Obligate anaerobe
C. Facultative anaerobe
D. Microaerophile
Answer: C
8. Which staining method demonstrates capsule clearly?
A. Ziehl–Neelsen stain
B. Albert stain
C. India ink preparation
D. Giemsa stain
Answer: C
9. Colony appearance of Klebsiella on nutrient agar is:
A. Dry and rough
B. Pigmented
C. Mucoid and glistening
D. Swarming
Answer: C
10. On MacConkey agar, Klebsiella pneumoniae forms:
A. Colorless colonies
B. Pale colonies
C. Pink mucoid colonies
D. Green colonies
Answer: C
11. Lactose fermentation by Klebsiella produces:
A. Acid only
B. Gas only
C. Acid and gas
D. No fermentation
Answer: C
12. Hemolysis on blood agar by Klebsiella is:
A. Alpha hemolysis
B. Beta hemolysis
C. Gamma hemolysis
D. Double zone hemolysis
Answer: C
13. Catalase reaction of Klebsiella pneumoniae is:
A. Negative
B. Weak positive
C. Positive
D. Variable
Answer: C
14. Oxidase test for Klebsiella is:
A. Positive
B. Negative
C. Weakly positive
D. Variable
Answer: B
15. Indole reaction of Klebsiella pneumoniae is:
A. Positive
B. Negative
C. Variable
D. Delayed positive
Answer: B
16. IMViC pattern of Klebsiella pneumoniae is:
A. ++––
B. ––++
C. +–+–
D. –+++
Answer: B
17. Methyl Red test in Klebsiella is:
A. Positive
B. Negative
C. Weak positive
D. Variable
Answer: B
18. Voges–Proskauer test in Klebsiella is:
A. Negative
B. Weak negative
C. Positive
D. Variable
Answer: C
19. Citrate utilization test in Klebsiella is:
A. Negative
B. Positive
C. Variable
D. Weak
Answer: B
20. Urease test in Klebsiella is:
A. Strong positive
B. Negative
C. Weak to moderate positive
D. Variable
Answer: C
21. TSI reaction of Klebsiella pneumoniae is:
A. K/A
B. A/A without gas
C. A/A with gas
D. K/K
Answer: C
22. Hydrogen sulfide production by Klebsiella:
A. Positive
B. Negative
C. Weak positive
D. Variable
Answer: B
23. The string test in Klebsiella is:
A. Negative
B. Weak
C. Positive
D. Variable
Answer: C
24. Klebsiella pneumoniae commonly causes:
A. Pharyngitis
B. Lobar pneumonia
C. Otitis media
D. Diphtheria
Answer: B
25. Sputum in Klebsiella pneumonia is classically:
A. Frothy
B. Purulent
C. Rusty
D. Currant jelly
Answer: D
26. Klebsiella pneumonia is common in:
A. Children
B. Alcoholics
C. Athletes
D. Pregnant women
Answer: B
27. Which infection is commonly associated with catheterization?
A. Pneumonia
B. UTI by Klebsiella
C. Meningitis
D. Osteomyelitis
Answer: B
28. Klebsiella pneumoniae is a major cause of:
A. Community skin infections
B. Nosocomial infections
C. Viral pneumonia
D. Fungal sepsis
Answer: B
29. Endotoxin of Klebsiella is:
A. Exotoxin
B. Capsule
C. Lipopolysaccharide
D. Enzyme
Answer: C
30. Siderophores help Klebsiella by:
A. Capsule formation
B. Iron acquisition
C. Motility
D. Sporulation
Answer: B
31. ESBL production confers resistance to:
A. Aminoglycosides
B. Tetracyclines
C. Third-generation cephalosporins
D. Vancomycin
Answer: C
32. Carbapenem resistance in Klebsiella is due to:
A. ESBL only
B. Carbapenemases
C. Capsule
D. Biofilm alone
Answer: B
33. NDM-1 is a type of:
A. ESBL
B. Carbapenemase
C. Efflux pump
D. Porin
Answer: B
34. Biofilm formation is important in:
A. Community infections
B. Device-associated infections
C. Viral infections
D. Skin flora
Answer: B
35. Klebsiella pneumoniae is WHO listed as:
A. Low priority pathogen
B. Medium priority pathogen
C. Priority MDR pathogen
D. Vaccine preventable pathogen
Answer: C
36. Specimen of choice for Klebsiella pneumonia diagnosis:
A. Blood
B. Urine
C. Sputum
D. CSF
Answer: C
37. Best media for differentiation of lactose fermentation:
A. Blood agar
B. Chocolate agar
C. MacConkey agar
D. TCBS agar
Answer: C
38. Automated identification of Klebsiella can be done by:
A. ELISA
B. VITEK / MALDI-TOF
C. Western blot
D. Immunofluorescence
Answer: B
39. Antimicrobial susceptibility testing is essential because of:
A. Slow growth
B. Capsule
C. Multidrug resistance
D. Poor staining
Answer: C
40. Normal habitat of Klebsiella is:
A. Skin
B. Oral cavity
C. Gastrointestinal tract
D. Blood
Answer: C
41. Mode of transmission in hospitals is mainly:
A. Airborne
B. Vector-borne
C. Hands of healthcare workers
D. Food
Answer: C
42. Most effective preventive measure is:
A. Vaccination
B. Hand hygiene
C. Probiotics
D. Antivirals
Answer: B
43. Vaccine against Klebsiella pneumoniae:
A. Available
B. Under trial only
C. Not available
D. Mandatory
Answer: C
44. Capsule antigen of Klebsiella is known as:
A. O antigen
B. H antigen
C. K antigen
D. Vi antigen
Answer: C
45. Klebsiella meningitis is more common in:
A. Healthy adults
B. Neonates and immunocompromised
C. Athletes
D. Smokers only
Answer: B
46. Which test differentiates Klebsiella from E. coli?
A. Catalase
B. Oxidase
C. Motility
D. Gram stain
Answer: C
47. Which Klebsiella species is indole-positive?
A. K. pneumoniae
B. K. oxytoca
C. K. aerogenes
D. K. rhinoscleromatis
Answer: B
48. ESBL genes are usually carried on:
A. Chromosome only
B. Ribosome
C. Plasmids
D. Capsule
Answer: C
49. Klebsiella shows resistance spread mainly by:
A. Mutation only
B. Vertical transmission
C. Horizontal gene transfer
D. Spore formation
Answer: C
50. Most important preventive strategy in ICU is:
A. High-dose antibiotics
B. Prolonged catheter use
C. Infection control & stewardship
D. Empirical therapy
Answer: C