
Introduction
- Acute diarrheal disease is a significant global health issue that can result from various infectious agents, including bacteria, viruses, and parasites.
- It is characterized by the sudden onset of diarrhea, which can lead to dehydration and, in severe cases, death, particularly among vulnerable populations such as children and the elderly.
- Timely and accurate laboratory diagnosis is essential for determining the cause of the diarrhea, guiding appropriate treatment, and implementing effective public health measures.
Epidemiology
1. Global Burden
-
Acute diarrheal disease is one of the most common infectious diseases worldwide.
-
It is a leading cause of morbidity and mortality in children under 5 years of age.
-
Developing countries bear the highest burden.
-
Millions of episodes occur annually, especially in low-income regions.
-
Mortality is mainly due to severe dehydration and electrolyte imbalance.
2. Geographic Distribution
-
Highly prevalent in:
-
South Asia
-
Sub-Saharan Africa
-
Latin America
-
-
Rural areas are more affected than urban areas.
-
Slum populations show higher incidence due to:
-
Overcrowding
-
Poor sanitation
-
Unsafe water
-
3. Age Distribution
-
Most affected group: Children below 5 years.
-
Infants (6 months–2 years) are at highest risk.
-
Elderly individuals are also vulnerable.
-
Immunocompromised patients show higher severity.
4. Seasonal Variation
-
More common during:
-
Summer season
-
Rainy season
-
-
Bacterial diarrhea peaks in summer.
-
Viral diarrhea (especially Rotavirus) is more common in winter in some regions.
-
Monsoon increases contamination of water sources.
5. Mode of Transmission
-
Fecal–oral route (most common).
-
Contaminated drinking water.
-
Contaminated food.
-
Poor hand hygiene.
-
Person-to-person contact (e.g., Norovirus outbreaks).
-
Flies acting as mechanical vectors.
6. Risk Factors
-
Lack of safe drinking water.
-
Poor sanitation facilities.
-
Open defecation.
-
Malnutrition.
-
Bottle feeding (instead of breastfeeding).
-
Incomplete vaccination (e.g., rotavirus vaccine).
-
Low socioeconomic status.
-
Overcrowding.
7. Causative Organisms in Epidemiology
A. Bacterial
-
Vibrio cholerae – Causes epidemics of cholera.
-
Escherichia coli – Common in traveler’s diarrhea.
-
Shigella dysenteriae – Causes bacillary dysentery.
-
Salmonella enterica – Foodborne outbreaks.
B. Viral
-
Rotavirus – Major cause in children.
-
Norovirus – Outbreaks in communities.
C. Parasitic
-
Entamoeba histolytica
-
Giardia lamblia
8. Outbreak Epidemiology
-
Occurs due to:
-
Contaminated water supply
-
Contaminated food
-
Natural disasters (floods)
-
-
Rapid spread in:
-
Schools
-
Hostels
-
Military camps
-
Refugee camps
-
-
Cholera outbreaks can affect thousands rapidly.
-
Prompt laboratory confirmation is essential for outbreak control.
9. Socioeconomic Impact
-
Increased hospital admissions.
-
Loss of school days in children.
-
Loss of productivity in adults.
-
Increased healthcare costs.
-
Nutritional deterioration in children.
10. Preventive Epidemiological Measures
-
Safe water supply.
-
Sanitation improvement programs.
-
Health education.
-
Breastfeeding promotion.
-
Vaccination (Rotavirus vaccine).
Etiology
Acute diarrhea may be caused by infectious and non-infectious agents.
A. Infectious Causes
1. Bacterial Causes
-
Vibrio cholerae
-
Causes cholera
-
Severe watery diarrhea
-
Epidemic outbreaks
-
-
Escherichia coli
-
ETEC → Traveler’s diarrhea
-
EHEC → Bloody diarrhea
-
EPEC → Infantile diarrhea
-
-
Shigella dysenteriae
-
Bacillary dysentery
-
Blood and mucus in stool
-
-
Salmonella enterica
-
Food-borne gastroenteritis
-
Fever with diarrhea
-
-
Clostridium perfringens
-
Food poisoning
-
Abdominal cramps
-
2. Viral Causes
-
Rotavirus
-
Most common in children
-
Severe watery diarrhea
-
-
Norovirus
-
Outbreaks in closed communities
-
-
Adenovirus (enteric type)
3. Parasitic Causes
-
Entamoeba histolytica
-
Amoebic dysentery
-
-
Giardia lamblia
-
Malabsorption diarrhea
-
-
Cryptosporidium
B. Non-Infectious Causes
-
Food intolerance
-
Drug-induced diarrhea (antibiotics)
-
Toxins
-
Malabsorption syndromes
Pathogenesis
The mechanism of diarrhoea depends on the causative agent.
A. Secretory Diarrhea
-
Caused by enterotoxin production.
-
Example: Vibrio cholerae
-
Mechanism:
-
Cholera toxin activates adenylate cyclase.
-
Increased cAMP in intestinal cells.
-
Increased chloride and water secretion.
-
Massive watery diarrhea.
-
-
Stool contains:
-
Large volume
-
No blood
-
-
Continues even during fasting.
B. Inflammatory (Invasive) Diarrhea
-
Caused by mucosal invasion.
-
Example:
-
Shigella dysenteriae
-
EHEC (E. coli)
-
-
Mechanism:
-
Invasion of intestinal epithelium.
-
Ulcer formation.
-
Inflammation.
-
-
Stool contains:
-
Blood
-
Mucus
-
Pus cells
-
-
Associated with fever.
C. Osmotic Diarrhea
-
Caused by malabsorption.
-
Undigested solutes retain water in intestine.
-
Stops during fasting.
-
Example:
-
Giardia infection.
-
D. Motility-Related Diarrhea
-
Increased intestinal motility.
-
Reduced contact time for absorption.
-
Seen in:
-
Irritable bowel syndrome.
-
Clinical Feature
Clinical features vary depending on severity and cause.
A. General Symptoms
-
Passage of loose or watery stools (≥3 per day).
-
Abdominal cramps.
-
Nausea.
-
Vomiting.
-
Fever (in invasive diarrhea).
-
Weakness.
B. Stool Characteristics
| Type | Features |
|---|---|
| Watery | Secretory diarrhea (e.g., cholera) |
| Bloody | Dysentery (Shigella, EHEC) |
| Mucoid | Inflammatory |
| Foul-smelling | Parasitic |
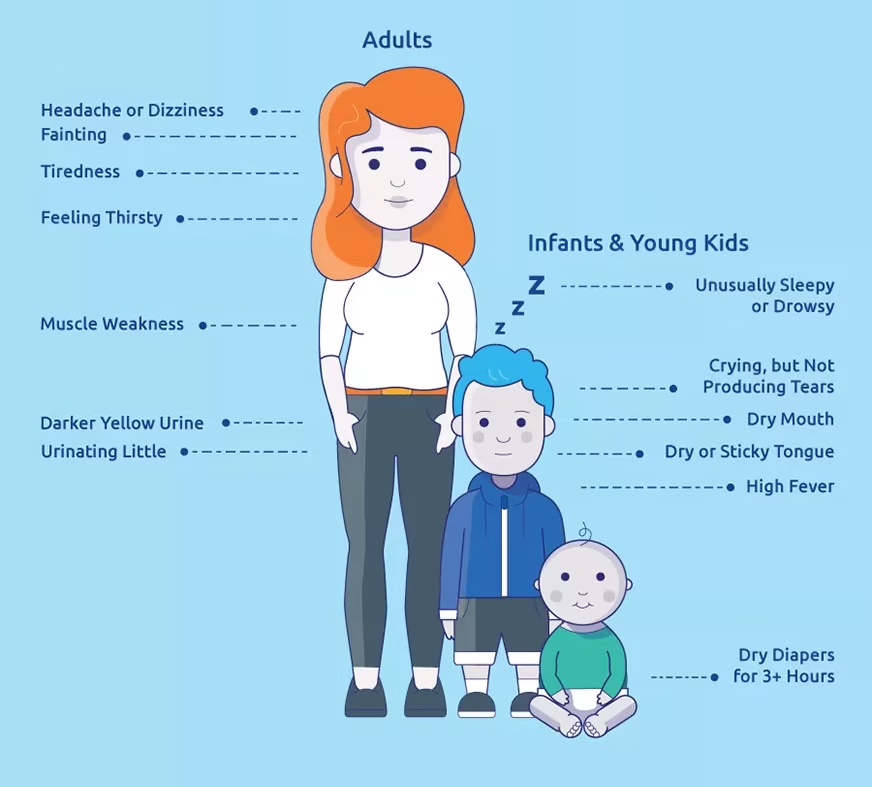
C. Signs of Dehydration
-
Dry mouth and tongue.
-
Sunken eyes.
-
Decreased skin turgor.
-
Tachycardia.
-
Hypotension.
-
Reduced urine output.
-
Lethargy.
D. Severity Classification
1. Mild
-
No dehydration.
-
Normal pulse and blood pressure.
2. Moderate
-
Thirsty.
-
Dry mucosa.
-
Slight tachycardia.
3. Severe
-
Shock.
-
Very low BP.
-
Cold extremities.
-
Altered consciousness.
E. Complications
-
Severe dehydration.
-
Electrolyte imbalance.
-
Hypokalemia.
-
Metabolic acidosis.
-
Renal failure.
-
Hemolytic uremic syndrome (EHEC).
-
Septicemia (Salmonella).
Laboratory Diagnosis
Specimen Collection
-
Fresh stool sample (preferred).
-
Rectal swab (if stool not available).
-
Suspected food sample (during outbreaks).
-
Blood sample (if systemic infection suspected).
B. Collection Guidelines
-
Collect before starting antibiotics.
-
Use sterile, wide-mouthed, leak-proof container.
-
Avoid contamination with urine.
-
Send to lab immediately.
-
If delay >2 hours → use Cary-Blair transport medium.
Macroscopic Examination of Stool
-
Color
-
Yellow/brown → Normal
-
Pale → Malabsorption
-
Red → Blood
-
Greenish → Infection
-
-
Consistency
-
Watery → Secretory diarrhea
-
Mucoid → Inflammatory
-
Bloody → Dysentery
-
-
Odor
-
Foul smell → Parasitic infection
-
-
Presence of:
-
Blood
-
Mucus
-
Worms
-
Microscopic Examination
-
Normal saline mount → Motility detection.
-
Iodine mount → Cyst identification.
Detects:
-
Ova
-
Cysts
-
Trophozoites
-
RBC
-
WBC
B. Interpretation
-
RBC present → Suggests invasive diarrhea
-
Example: Shigella dysenteriae
-
-
WBC present → Inflammatory diarrhea
-
No RBC/WBC → Secretory diarrhea
-
Example: Vibrio cholerae
-
-
Ova/Cysts present → Parasitic infection
-
Entamoeba histolytica
-
Giardia lamblia
-
Stool Culture
A. Indications
-
Severe diarrhea.
-
Bloody diarrhea.
-
High fever.
-
Suspected outbreak.
-
Immunocompromised patient.
B. Culture Media Used
| Organism | Media |
|---|---|
| Escherichia coli | MacConkey agar |
| Salmonella enterica | XLD agar |
| Shigella dysenteriae | SS agar |
| Vibrio cholerae | TCBS agar |

C. Colony Characteristics
-
Lactose fermenters → Pink colonies (MacConkey).
-
Non-lactose fermenters → Colorless colonies.
-
Yellow colonies on TCBS → Vibrio cholerae.
-
Black-centered colonies on XLD → Salmonella (H₂S production).
Biochemical Tests
-
TSI (Triple Sugar Iron test).
-
Indole test.
-
Citrate test.
-
Urease test.
-
Oxidase test (Vibrio positive).
-
Coagulase (for Staphylococcus in food poisoning).
Serological Tests
-
Widal test → Salmonella.
-
Rapid antigen test → Rotavirus.
-
ELISA → Viral antigens.
Molecular Diagnosis
-
PCR → Detect bacterial toxin genes.
-
Multiplex PCR panels → Detect multiple pathogens.
-
Real-time PCR → Rapid diagnosis.
Advantages:
-
High sensitivity.
-
Rapid results.
Antibiotic Sensitivity Testing (AST)
-
Performed after bacterial isolation.
-
Kirby-Bauer disk diffusion method.
-
Guides appropriate antibiotic therapy.
-
Important in resistant infections.
Special Investigations
-
Electrolyte estimation (Na⁺, K⁺).
-
Blood urea and creatinine (renal function).
-
ABG (metabolic acidosis).
-
Complete blood count (CBC).
Interpretation of Laboratory Findings
| Finding | Suggests |
|---|---|
| Watery stool, no WBC | Secretory diarrhea |
| RBC + WBC | Invasive diarrhea |
| Ova/Cyst | Parasitic infection |
| Positive culture | Bacterial cause |
Treatment
Rehydration Therapy
A. Oral Rehydration Therapy (ORT)
-
First-line treatment in most cases.
-
Prevents dehydration-related mortality.
-
Can be given at home.
Composition of WHO ORS (Low Osmolarity)
-
Sodium chloride
-
Glucose
-
Potassium chloride
-
Trisodium citrate
Mechanism
-
Glucose enhances sodium absorption.
-
Sodium absorption promotes water absorption.
-
Corrects dehydration and electrolyte imbalance.
B. Indications for ORS
-
Mild dehydration.
-
Moderate dehydration.
-
Continued diarrhea after IV therapy.
Intravenous (IV) Fluid Therapy
-
Severe dehydration.
-
Shock.
-
Persistent vomiting.
-
Unable to drink orally.
Fluids Used
-
Ringer lactate (preferred).
-
Normal saline.
Monitoring
-
Pulse rate.
-
Blood pressure.
-
Urine output.
-
Electrolytes.
Zinc Supplementation (Especially in Children)
-
Recommended in children under 5 years.
-
Dose:
-
10 mg/day (<6 months)
-
20 mg/day (>6 months)
-
-
Duration: 14 days.
-
Benefits:
-
Reduces duration of diarrhea.
-
Reduces recurrence.
-
Antibiotic Therapy
Indications
-
Cholera
-
Vibrio cholerae
-
-
Bacillary dysentery
-
Shigella dysenteriae
-
-
Severe Salmonella infection
-
Salmonella enterica
-
-
Immunocompromised patients.
Not Indicated In
-
Viral diarrhea (e.g., Rotavirus).
-
Mild watery diarrhea.
Important Note
-
Overuse leads to antibiotic resistance.
-
Antibiotics must be based on culture and sensitivity report.
Anti-diarrheal Drugs
-
Generally NOT recommended in children.
-
Avoid in dysentery (bloody diarrhea).
-
May prolong infection.
Nutritional Management
-
Continue breastfeeding.
-
Do not stop feeding.
-
Give light, easily digestible diet.
-
Avoid fatty and spicy food.
-
Prevent malnutrition.
Management of Complications
-
Severe dehydration → IV fluids.
-
Hypokalemia → Potassium correction.
-
Metabolic acidosis → Correct fluids.
-
Shock → Emergency management.
Prevention
1. Primary Prevention
A. Safe Water Supply
-
Boiled water.
-
Chlorinated water.
-
Proper water storage.
B. Sanitation
-
Proper sewage disposal.
-
Use of toilets.
-
Avoid open defecation.
C. Hand Hygiene
-
Wash hands before eating.
-
Wash hands after toilet use.
-
Use soap and clean water.
D. Food Hygiene
-
Cook food properly.
-
Avoid stale food.
-
Cover food to prevent flies.
-
Wash fruits and vegetables properly.
2. Immunization
-
Rotavirus vaccine for infants.
-
Cholera vaccine in endemic areas.
Vaccination reduces:
-
Severity
-
Hospitalization
-
Mortality
3. Breastfeeding Promotion
-
Exclusive breastfeeding for 6 months.
-
Protects against infections.
-
Provides immunity.
4. Health Education
-
Community awareness programs.
-
School health programs.
-
Teaching ORS preparation at home.
5. Surveillance & Outbreak Control
-
Early reporting of cases.
-
Laboratory confirmation.
-
Isolation during outbreaks.
-
Disinfection of contaminated sources.
MCQs
1. Acute diarrhea is defined as diarrhea lasting less than:
A. 7 days
B. 10 days
C. 14 days
D. 30 days
Answer: C
2. The most common cause of acute diarrhea in children is:
A. Rotavirus
B. Salmonella
C. Giardia
D. Shigella
Answer: A
3. The major cause of death in acute diarrhea is:
A. Fever
B. Vomiting
C. Dehydration
D. Abdominal pain
Answer: C
4. Rice-water stool is characteristic of:
A. Shigella
B. Vibrio cholerae
C. Salmonella
D. E. coli
Answer: B
5. Bloody diarrhea is most commonly caused by:
A. Rotavirus
B. Norovirus
C. Shigella dysenteriae
D. Vibrio
Answer: C
6. The most important treatment in ADD is:
A. Antibiotics
B. ORS
C. Steroids
D. Antacids
Answer: B
7. ORS works by enhancing absorption of:
A. Protein
B. Fat
C. Sodium and water
D. Iron
Answer: C
8. Severe dehydration requires:
A. ORS only
B. IV fluids
C. Antibiotics only
D. Zinc only
Answer: B
9. TCBS agar is used to isolate:
A. Salmonella
B. Vibrio cholerae
C. Shigella
D. E. coli
Answer: B
10. RBC in stool suggests:
A. Secretory diarrhea
B. Viral infection
C. Invasive diarrhea
D. Osmotic diarrhea
Answer: C
11. The most common mode of transmission is:
A. Airborne
B. Vector-borne
C. Fecal-oral route
D. Blood transfusion
Answer: C
12. Zinc supplementation is recommended for:
A. Adults
B. Children
C. Elderly only
D. Pregnant women
Answer: B
13. Lactose fermenting colonies on MacConkey agar appear:
A. Colorless
B. Pink
C. Black
D. Green
Answer: B
14. Non-lactose fermenter:
A. Salmonella enterica
B. E. coli
C. Klebsiella
D. Enterobacter
Answer: A
15. Secretory diarrhea continues during:
A. Feeding
B. Fasting
C. Exercise
D. Sleep
Answer: B
16. The toxin of Vibrio cholerae increases:
A. cAMP
B. cGMP
C. ATP
D. DNA
Answer: A
17. Most rapid diagnostic method:
A. Culture
B. Microscopy
C. PCR
D. Wet mount
Answer: C
18. Ova and cyst in stool indicate:
A. Viral infection
B. Bacterial infection
C. Parasitic infection
D. Chemical poisoning
Answer: C
19. Hypokalemia is a complication of:
A. Mild diarrhea
B. Severe diarrhea
C. Constipation
D. IBS
Answer: B
20. Transport medium for stool:
A. Nutrient broth
B. Cary-Blair medium
C. Blood agar
D. TCBS
Answer: B
21. Most common viral outbreak agent:
A. Norovirus
B. Rotavirus
C. Influenza
D. Adenovirus
Answer: A
22. Black-centered colonies on XLD suggest:
A. E. coli
B. Vibrio
C. Salmonella
D. Shigella
Answer: C
23. Decreased skin turgor indicates:
A. Fever
B. Dehydration
C. Hypertension
D. Anemia
Answer: B
24. ORS should be prepared with:
A. Hot milk
B. Juice
C. Clean water
D. Tea
Answer: C
25. Most common age group affected:
A. Adults
B. Elderly
C. Under 5 years
D. Teenagers
Answer: C
26. Fever with diarrhea suggests:
A. Viral infection
B. Invasive bacterial infection
C. Chemical poisoning
D. Osmotic diarrhea
Answer: B
27. Indole positive organism:
A. Escherichia coli
B. Salmonella
C. Shigella
D. Vibrio
Answer: A
28. Severe dehydration may lead to:
A. Hypertension
B. Shock
C. Diabetes
D. Asthma
Answer: B
29. Most important preventive measure:
A. Steroids
B. Vaccination only
C. Hand washing
D. Surgery
Answer: C
30. Rotavirus mainly affects:
A. Adults
B. Children
C. Elderly
D. Pregnant women
Answer: B
31. Blood and mucus in stool is typical of:
A. Cholera
B. Dysentery
C. Viral diarrhea
D. Osmotic diarrhea
Answer: B
32. Cholera outbreaks are common after:
A. Earthquake
B. Flood
C. Winter
D. Drought
Answer: B
33. Hypotension in ADD indicates:
A. Mild disease
B. Severe dehydration
C. Recovery
D. Constipation
Answer: B
34. MacConkey agar differentiates bacteria based on:
A. Hemolysis
B. Lactose fermentation
C. Motility
D. Spore formation
Answer: B
35. Antibiotics are NOT required in:
A. Cholera
B. Dysentery
C. Rotavirus infection
D. Severe Salmonella
Answer: C
36. Most common complication in children:
A. Malnutrition
B. Cancer
C. Hypertension
D. Arthritis
Answer: A
37. WBC in stool indicates:
A. Secretory diarrhea
B. Inflammatory diarrhea
C. Viral infection
D. Osmotic diarrhea
Answer: B
38. Major electrolyte lost in diarrhea:
A. Iron
B. Calcium
C. Sodium
D. Iodine
Answer: C
39. Best initial management in mild ADD:
A. Antibiotics
B. ORS
C. IV fluids
D. Surgery
Answer: B
40. Stool culture is indicated in:
A. Mild watery diarrhea
B. Bloody diarrhea
C. IBS
D. Constipation
Answer: B
41. Hypovolemic shock results from:
A. Fever
B. Dehydration
C. Vomiting only
D. Hypertension
Answer: B
42. Exclusive breastfeeding protects against:
A. Hypertension
B. Diarrhea
C. Diabetes
D. Cancer
Answer: B
43. Motility-related diarrhea occurs due to:
A. Increased intestinal movement
B. Toxin
C. Infection
D. Ulcer
Answer: A
44. EHEC may cause:
A. Cholera
B. Hemolytic uremic syndrome
C. Tuberculosis
D. Hepatitis
Answer: B
45. The gold standard for bacterial identification:
A. Microscopy
B. Culture
C. PCR
D. Serology
Answer: B
46. Shock in ADD requires:
A. ORS only
B. Immediate IV fluids
C. Zinc
D. Antacids
Answer: B
47. Most common transmission in children:
A. Blood
B. Fecal-oral
C. Air
D. Vector
Answer: B
48. Secretory diarrhea is characterized by:
A. Blood in stool
B. Large watery stool
C. Severe pain
D. Ulcer
Answer: B
49. Dysentery is defined by:
A. Watery stool
B. Loose stool only
C. Blood and mucus in stool
D. Constipation
Answer: C
50. The cornerstone of management of ADD is:
A. Steroids
B. ORS
C. Antibiotics
D. Surgery
Answer: B