Introduction
- Intestinal protozoa infections caused by Entamoeba histolytica (responsible for amoebiasis) and Giardia lamblia (causing giardiasis) are significant public health concerns worldwide.
- These infections result from protozoan parasites that inhabit the gastrointestinal tract, leading to diarrhea, abdominal discomfort, malabsorption, and, in severe cases, life-threatening complications.
- Both organisms share similarities in transmission, primarily via the fecal-oral route, but differ in their life cycles, pathogenesis, and clinical manifestations.
- This article explains the introduction, geographical distribution, habitat, morphology, life cycle, transmission mode, incubation time, pathogenesis, laboratory diagnosis, and treatment of these two major intestinal protozoan infections.
Geographical Distribution
Amoeba (Entamoeba histolytica)
-
- Worldwide distribution, but most prevalent in tropical and subtropical regions with poor sanitation.
- The highest prevalence is in South Asia, Africa, and Central and South America.
- Common in travelers, refugees, and individuals in institutionalized settings.
Giardia (Giardia lamblia)
-
- Found globally, with higher prevalence in low-income regions where sanitation is inadequate.
- Endemic in parts of Africa, South Asia, and Latin America.
- Outbreaks often occur in developed countries due to exposure to contaminated water supplies or recreational water.
Habitat
Amoeba
-
- Trophozoite stage: Resides in the large intestine, feeding on bacteria and tissue.
- Cyst stage: Found in the colon and excreted in feces, surviving in the environment for extended periods.
Giardia
-
- Trophozoite stage: Attaches to the mucosa of the small intestine, primarily the duodenum and jejunum.
- Cyst stage: Forms in the colon and is shed in feces, surviving in external environments such as water and soil.
Morphology
Amoeba (Entamoeba histolytica)
-
- Trophozoite:
- Amoeboid shape, measuring 10–60 µm.
- Contains a single nucleus with a central karyosome.
- Engulfs red blood cells (erythrophagocytosis), a diagnostic feature.
- Cyst:
- Spherical, 10–20 µm in diameter.
- Contains 1–4 nuclei and chromatoid bodies.
- Trophozoite:
Giardia (Giardia lamblia)
-
- Trophozoite:
- Pear-shaped, 9–21 µm long and 5–15 µm wide.
- Binucleate with a ventral adhesive disc and four pairs of flagella.
- Cyst:
- Oval, 8–14 µm in length, with a thick wall.
- Contains four nuclei when mature.
- Trophozoite:
Life Cycle
Amoeba
-
- Ingestion: Cysts are ingested via contaminated water, food, or hands.
- Excystation: Cysts release trophozoites in the small intestine.
- Colonization: Trophozoites colonize the colon, feeding on host tissue.
- Encystation: Trophozoites form cysts in the large intestine.
- Excretion: Cysts are passed in feces and remain infectious in the environment.
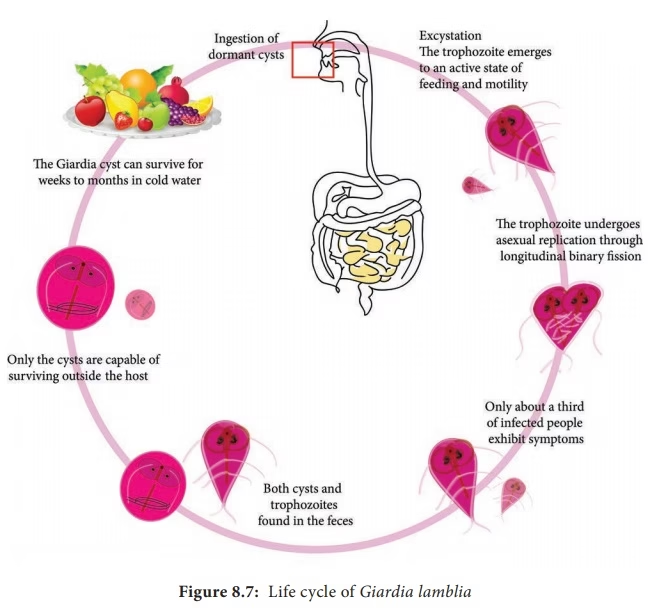
Giardia
-
- Ingestion: Cysts are ingested through contaminated water, food, or direct contact.
- Excystation: Gastric acid stimulates the release of trophozoites in the duodenum.
- Colonization: Trophozoites attach to the intestinal mucosa and multiply by binary fission.
- Encystation: Trophozoites form cysts in the colon.
- Excretion: Cysts are excreted in feces and survive in the environment.
Mode of Transmission
Both Entamoeba histolytica and Giardia lamblia share similar transmission routes:
-
- Fecal-oral route:
- Ingestion of contaminated food, water, or hands.
- Common in areas with poor sanitation and hygiene.
- Person-to-person contact:
- Transmission in daycare centers, households, and institutional settings.
- Sexual transmission via oral-anal contact.
- Zoonotic transmission (Giardia only):
- Contact with infected animals, such as beavers or dogs.
- Fecal-oral route:
Incubation Time
-
- Amoeba (Entamoeba histolytica): 1–4 weeks after ingestion of cysts.
- Giardia (Giardia lamblia): 1–2 weeks (commonly 7–10 days).
Pathogenesis
Amoeba
-
- Trophozoites invade the colonic mucosa, causing necrosis and ulceration.
- Severe cases lead to extraintestinal spread, especially to the liver (amoebic liver abscess).
- Clinical manifestations:
- Intestinal: Dysentery, abdominal pain, and bloody diarrhea.
- Extraintestinal: Liver abscess (fever, right upper quadrant pain), pleuropulmonary amoebiasis, and brain involvement (rare).
Giardia
-
- Trophozoites attach to the small intestinal mucosa, disrupting the epithelial barrier and causing malabsorption.
- Villous atrophy and enzyme deficiencies (e.g., lactase) exacerbate symptoms.
- Clinical manifestations:
- Acute: Watery diarrhea, bloating, flatulence, nausea, and abdominal cramps.
- Chronic: Malabsorption, weight loss, and fatigue.
- Asymptomatic carriers: Shed cysts without symptoms.
Laboratory Diagnosis
Laboratory diagnosis of Entamoeba histolytica is essential for confirming amoebiasis and differentiating it from other causes of diarrhea and dysentery. Diagnosis is based on the detection of trophozoites, cysts, antigens, antibodies, or parasite DNA in clinical specimens.
1. Stool Examination
- Stool microscopy is the most common and widely used method for diagnosing intestinal amoebiasis.
Specimen Collection
- Fresh stool sample should be collected in a clean, dry container.
- Multiple stool samples (at least three specimens collected on different days) are recommended because cyst shedding may be intermittent.
- Diarrheal stool should be examined immediately to observe motile trophozoites.
Macroscopic Examination
The stool may show:
- Blood
- Mucus
- Semi-formed or loose consistency
- Foul odor
In amoebic dysentery, stools are often scanty and contain blood and mucus.
Microscopic Examination
A. Saline Wet Mount
- Fresh stool is examined in normal saline.
Findings
Trophozoites
- Motile amoeboid organisms
- Finger-like pseudopodia
- Single nucleus
- Ingested red blood cells may be seen
Significance
The presence of trophozoites containing ingested RBCs is considered diagnostic of Entamoeba histolytica.
B. Iodine Wet Mount
- Used mainly for cyst detection.
Findings
- Round cysts
- One to four nuclei
- Chromatoid bodies
Advantages
- Better visualization of nuclear structures
- Useful for identifying cyst morphology
2. Concentration Techniques
- Concentration methods improve the detection of cysts when parasites are present in small numbers.
Common Methods
Formalin-Ether Sedimentation Technique
- Most commonly used concentration method.
- Concentrates cysts effectively.
Zinc Sulfate Flotation Method
Useful for recovery of cysts from stool specimens.
Advantages
Increased sensitivity
Better parasite recovery
3. Permanent Stained Smears
- Permanent staining provides detailed morphological features of trophozoites and cysts.
Trichrome Stain
Findings
- Nucleus clearly visible
- Cytoplasmic details well demonstrated
Advantages
- Most commonly used permanent stain
Iron Hematoxylin Stain
Advantages
- Excellent nuclear detail
- Useful for species identification
4. Sigmoidoscopy and Colonic Biopsy
- In suspected invasive amoebiasis, direct visualization of intestinal lesions may be performed.
Findings
- Flask-shaped ulcers
- Inflamed mucosa
- Tissue necrosis
Biopsy Examination
Demonstrates:
- Trophozoites invading tissue
- Inflammatory reaction
5. Examination of Aspirated Material
- Particularly useful in amoebic liver abscess.
Liver Abscess Aspiration
Aspirated material typically appears:
- Thick
- Brown
- Odorless
It is often described as “anchovy sauce” pus.
Microscopic Findings
- Trophozoites may be found at the wall of the abscess.
- They are rarely seen in the central pus.
6. Antigen Detection Tests
- These tests detect specific Entamoeba histolytica antigens in stool or serum.
Methods
ELISA (Enzyme-Linked Immunosorbent Assay)
Advantages
- Highly sensitive
- Highly specific
- Rapid diagnosis
Uses
- Detection of intestinal amoebiasis
- Detection of liver abscess
Rapid Immunochromatographic Tests
Advantages
- Quick results
- Easy to perform
- Suitable for routine laboratories
7. Serological Tests
- Useful especially in extraintestinal amoebiasis.
Common Tests
ELISA
- Indirect Hemagglutination Test (IHA)
- Indirect Fluorescent Antibody Test (IFA)
- Latex Agglutination Test
Significance
Positive serology strongly supports:
- Amoebic liver abscess
- Extraintestinal amoebiasis
Antibodies may remain positive for months or years after infection.
8. Molecular Diagnosis
- Polymerase Chain Reaction (PCR)
PCR detects parasite DNA in:
- Stool
- Tissue samples
- Abscess material
Advantages
- Highly sensitive
- Highly specific
- Differentiates E. histolytica from nonpathogenic species such as E. dispar
Limitations
- Expensive
- Requires specialized laboratory facilities
9. Imaging Studies
- Used mainly for extraintestinal amoebiasis.
Ultrasonography (USG)
Can detect:
- Amoebic liver abscess
- Size and location of lesions
CT Scan and MRI
Useful for:
- Deep liver abscesses
- Brain involvement
- Complicated disease
Summary of Laboratory Diagnosis
| Investigation | Findings |
|---|---|
| Stool Microscopy | Trophozoites and cysts |
| Saline Wet Mount | Motile trophozoites with ingested RBCs |
| Iodine Mount | Cysts with nuclei |
| Concentration Techniques | Increased cyst recovery |
| Trichrome Stain | Detailed morphology |
| Sigmoidoscopy | Flask-shaped ulcers |
| Liver Abscess Aspiration | Anchovy sauce pus |
| ELISA | Antigen detection |
| Serology | Antibody detection |
| PCR | Detection of parasite DNA |
| Ultrasonography | Liver abscess detection |
Treatment
Amoeba
-
- Amoebic colitis or dysentery:
- Metronidazole (750 mg three times daily for 7–10 days) or Tinidazole (2 g daily for 3 days).
- Asymptomatic cyst carriers:
- Paromomycin or iodoquinol to eliminate cysts.
- Amoebic liver abscess:
- Drainage in severe cases, combined with metronidazole or tinidazole.
- Amoebic colitis or dysentery:
Giardia
-
- First-line treatment:
- Metronidazole (250 mg three times daily for 5–7 days) or Tinidazole (single 2 g dose).
- Alternative drugs:
- Nitazoxanide, Albendazole, or Furazolidone for resistant cases or intolerance to metronidazole.
- Supportive care:
- Rehydration therapy and dietary modifications (e.g., avoiding lactose).
- First-line treatment:
Prevention and Control
-
- Improve sanitation:
- Access to clean water and proper sewage disposal.
- Promote hygiene:
- Regular handwashing and proper food handling.
- Water treatment:
- Boiling, filtration, or chemical disinfection of drinking water.
- Public health measures:
- Education campaigns and screening in high-risk populations.
- Improve sanitation: