
Introduction
-
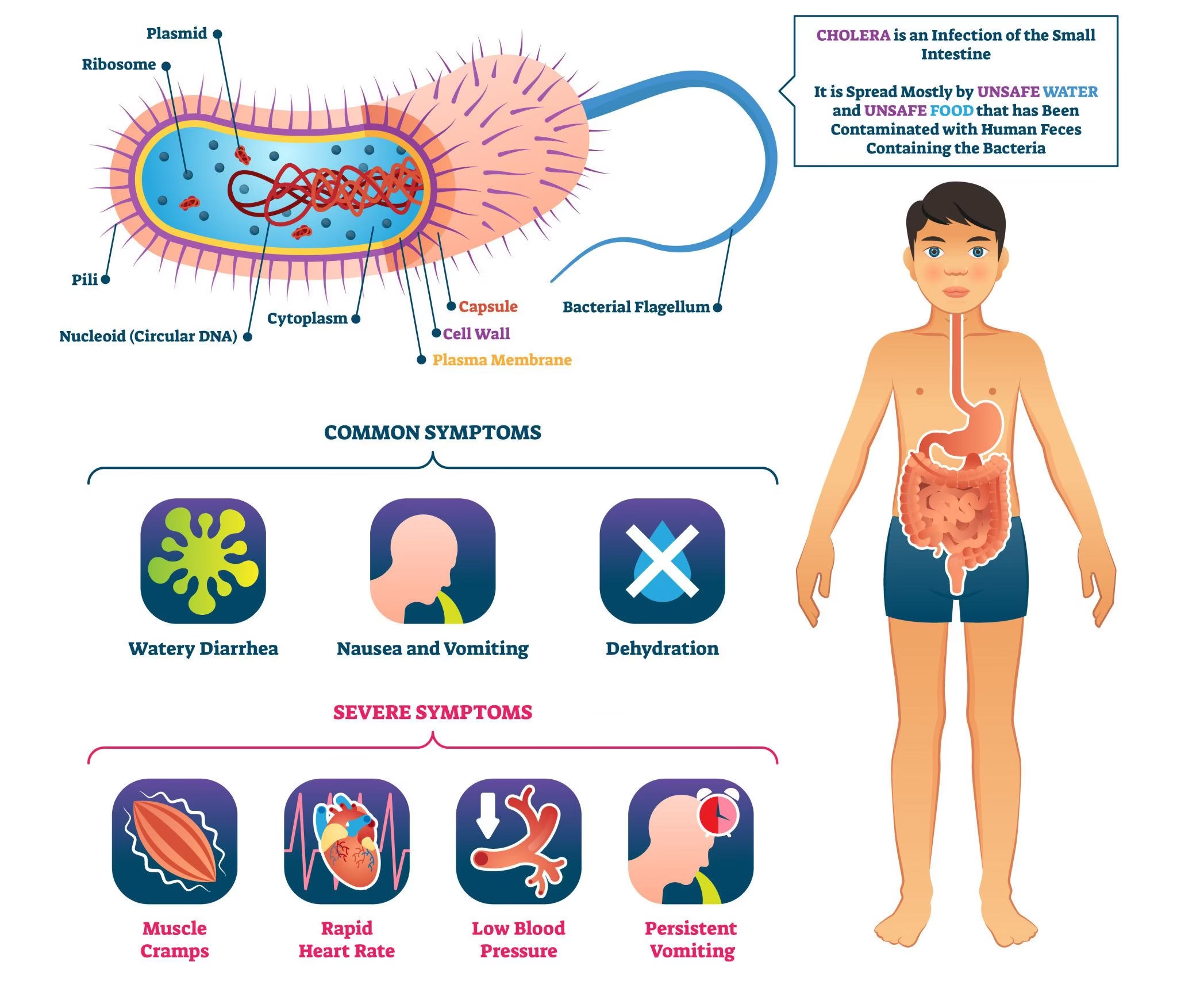
Cholera is an acute, severe diarrheal disease caused by the bacterium Vibrio cholerae.
-
It is characterized by profuse watery diarrhea, which can rapidly lead to severe dehydration and death if not treated promptly.
-
The disease is primarily transmitted through contaminated water and food, making it closely associated with poor sanitation and hygiene.
-
Cholera remains a major public health problem in many developing countries, especially during outbreaks and natural disasters.
-
Rapid progression of illness necessitates early diagnosis and immediate treatment.
-
Laboratory diagnosis plays a critical role in confirming cases, guiding therapy, and implementing effective outbreak control measures.
-
Preventive strategies such as safe water supply, sanitation, hygiene, and vaccination are essential for reducing cholera-related morbidity and mortality.

Epidemiology and Transmission of Cholera
Epidemiology
-
Cholera is a global public health problem, mainly affecting developing and underdeveloped countries.
-
It is endemic in parts of:
-
South and Southeast Asia
-
Sub-Saharan Africa
-
Latin America
-
-
Periodic epidemics and pandemics occur, especially after:
-
Floods, cyclones, earthquakes
-
Wars, refugee crises, and population displacement
-
Breakdown of water supply and sewage systems
-
-
High-risk settings include:
-
Urban slums
-
Refugee camps
-
Areas with poor sanitation and unsafe drinking water
-
-
All age groups are affected, but children and malnourished individuals are at higher risk of severe disease.
Transmission
Cholera is transmitted by the fecal–oral route, primarily through ingestion of contaminated water or food.
Major Modes of Transmission
-
Contaminated drinking water
-
Most common and important route
-
Occurs due to sewage contamination of water sources
-
-
Contaminated food
-
Raw or undercooked seafood (especially shellfish)
-
Food prepared with contaminated water
-
Street food with poor hygiene practices
-
-
Poor personal hygiene
-
Inadequate handwashing after defecation
-
Improper food handling
-
Reservoir and Source of Infection
-
Humans are the primary reservoir
-
Infected individuals (symptomatic or asymptomatic) shed large numbers of organisms in stool
-
Contaminated water bodies can act as temporary environmental reservoirs
Factors Favoring Transmission
-
Poor sanitation and open defecation
-
Unsafe water supply
-
Overcrowding
-
Low socioeconomic conditions
-
Lack of health education
Seasonal Variation
-
Cholera shows seasonal peaks, often:
-
During rainy seasons
-
In warmer months when water contamination is common
-
Pathogenesis
The pathogenesis of cholera is non-invasive and toxin-mediated, leading to massive fluid loss without intestinal inflammation.
1. Entry and Colonization
-
Infection occurs by ingestion of Vibrio cholerae through contaminated food or water
-
A large inoculum is usually required, but reduced gastric acidity (achlorhydria, antacids) lowers the infectious dose
-
The organism survives gastric acid and reaches the small intestine
2. Adherence to Intestinal Mucosa
-
Bacteria adhere to the epithelial cells of the small intestine using:
-
Toxin-coregulated pilus (TCP)
-
-
There is no invasion of intestinal mucosa and no tissue destruction
3. Production of Cholera Toxin
-
Vibrio cholerae produces cholera toxin (CT), an AB₅ exotoxin
-
B subunit binds to GM1 ganglioside receptors on enterocytes
-
A subunit enters the cell and activates adenylate cyclase
-
4. Increased cAMP Levels
-
Activation of adenylate cyclase → ↑ intracellular cAMP
-
cAMP causes:
-
Increased chloride secretion
-
Inhibition of sodium absorption
-
Massive efflux of water and electrolytes into intestinal lumen
-
5. Resulting Effect
-
Profuse watery diarrhea
-
Severe dehydration and electrolyte imbalance
-
No fever or inflammatory response (non-inflammatory diarrhea)
Clinical Features
The clinical presentation ranges from asymptomatic infection to severe, life-threatening dehydration.
1. Incubation Period
-
Usually 1–5 days
-
Shorter incubation is associated with severe disease
2. Diarrhea
-
Sudden onset of profuse, painless watery diarrhea
-
Stools described as “rice-water stools”
-
Colorless, cloudy fluid with flecks of mucus
-
No blood or pus
-
3. Vomiting
-
Frequent and effortless
-
Contributes to rapid fluid loss
4. Dehydration
Signs of dehydration appear rapidly and include:
-
Thirst
-
Sunken eyes
-
Dry tongue and skin
-
Reduced urine output (oliguria)
-
Loss of skin turgor
5. Electrolyte Imbalance
-
Loss of sodium, potassium, bicarbonate
-
Leads to:
-
Muscle cramps (especially calves)
-
Metabolic acidosis
-
Weakness
-
6. Severe Disease (Cholera Gravis)
-
Hypovolemic shock
-
Rapid pulse, low blood pressure
-
Cold clammy skin
-
Cyanosis
-
Anuria
-
If untreated → death within hours
7. Absence of Certain Features
-
Usually no fever
-
No abdominal pain
-
No blood or leukocytes in stool
Laboratory Diagnosis
Laboratory confirmation is crucial for early treatment, outbreak detection, and public health surveillance.
1. Specimen Collection
-
Fresh stool sample (preferred) or rectal swab
-
Collected before antibiotic therapy
-
If delay is expected, transport in Cary–Blair medium
-
Samples should be processed promptly to preserve viability
2. Microscopic Examination
-
Hanging drop / wet mount:
-
Shows rapid darting motility
-
-
Motility is inhibited by specific antisera
-
Useful as a rapid presumptive test during outbreaks
3. Culture Methods (Gold Standard)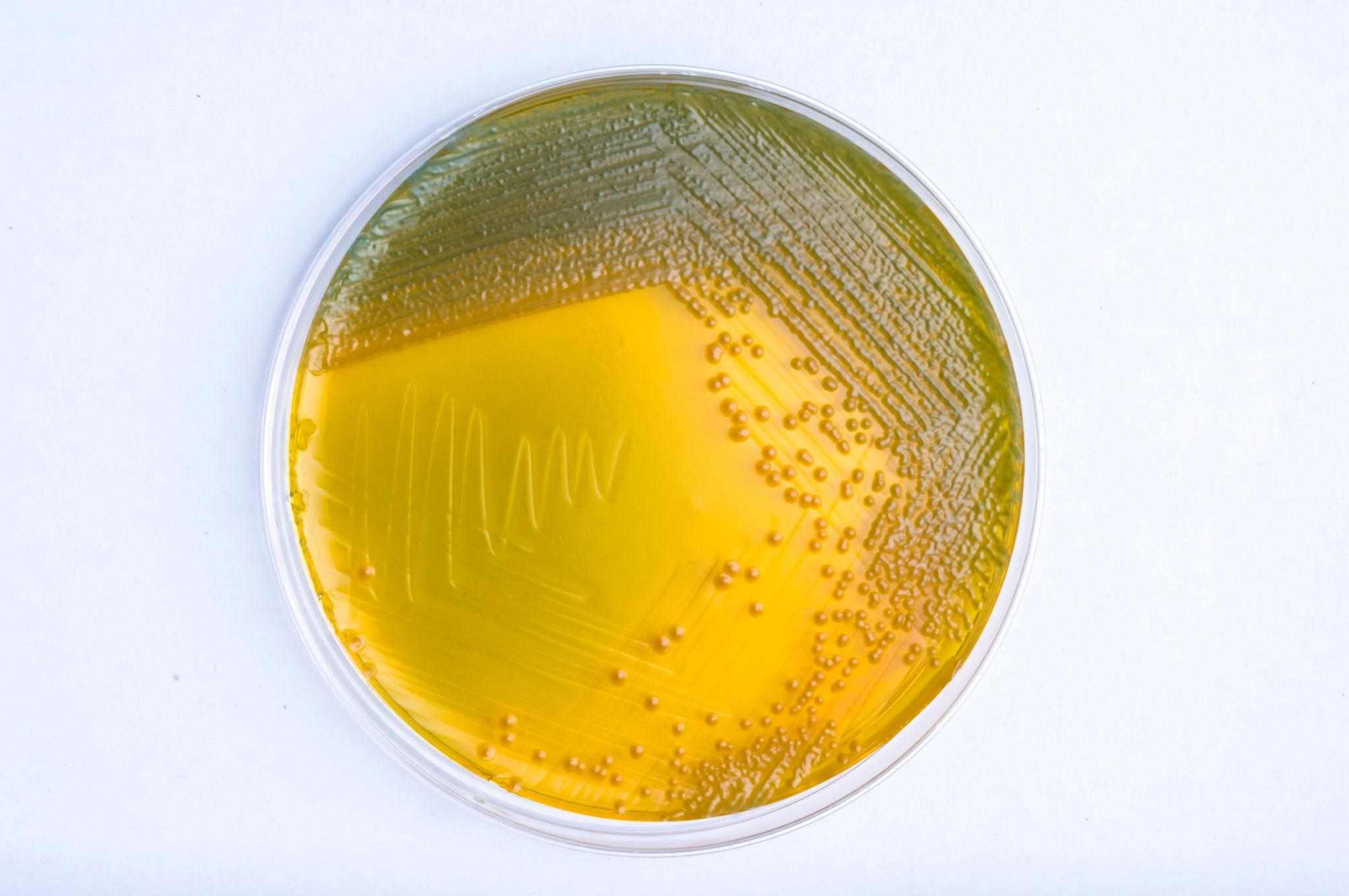
Step-wise approach:
-
Enrichment:
-
Alkaline peptone water (pH ~8.5)
-
-
Selective plating:
-
TCBS agar (Thiosulfate–Citrate–Bile salts–Sucrose)
-
-
Colony characteristics:
-
Large yellow colonies due to sucrose fermentation
-
4. Biochemical Identification
-
Oxidase positive
-
Ferments sucrose
-
Indole positive
-
String test positive (mucoid string with sodium deoxycholate)
5. Serological Identification
-
Slide agglutination using specific antisera
-
Detection of:
-
O1 (El Tor, Classical biotypes)
-
O139 (epidemic potential)
-
-
Important for epidemiological tracking
6. Rapid Diagnostic Tests (RDTs)
-
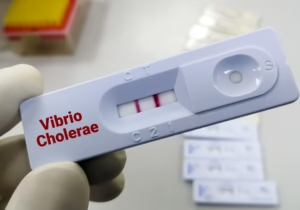
Immunochromatographic dipstick tests
-
Detect cholera antigens directly from stool
-
Advantages:
-
Fast (results in minutes)
-
Useful in field and outbreak settings
-
-
Limitation:
-
Less specific than culture
-
7. Molecular Methods
-
PCR for toxin and species-specific genes
-
Highly sensitive and specific
-
Used mainly in reference and research laboratories
Public Health Importance
-
Cholera can cause explosive outbreaks affecting thousands within days
-
Laboratory diagnosis helps in:
-
Early outbreak detection
-
Confirmation of suspected cases
-
Monitoring spread and severity
-
Planning control strategies
-
Public Health Aspects
-
One infected person can contaminate large water sources
-
Asymptomatic carriers play a role in transmission
-
High case fatality if untreated, but <1% with proper care
Prevention and Control
1. Water Safety
-
Provision of safe drinking water
-
Boiling or chlorination of water
-
Protection of water sources from sewage contamination
2. Sanitation Measures
-
Proper sewage disposal
-
Use of sanitary latrines
-
Prevention of open defecation
3. Food Hygiene
-
Proper cooking of food
-
Avoidance of raw seafood
-
Clean food handling practices
4. Personal Hygiene
-
Handwashing with soap after defecation and before meals
-
Hygiene education in communities
5. Case Management
-
Prompt oral rehydration therapy (ORT)
-
Intravenous fluids in severe dehydration
-
Antibiotics to reduce duration and shedding
6. Surveillance and Outbreak Control
-
Reporting of cases
-
Laboratory confirmation
-
Isolation of cases where feasible
-
Disinfection of stools and contaminated materials
7. Vaccination
-
Oral cholera vaccines in:
-
Endemic areas
-
High-risk populations
-
During outbreaks as preventive strategy
-
MCQs
1. Cholera is caused by which organism?
A. Escherichia coli
B. Salmonella typhi
C. Vibrio cholerae
D. Shigella dysenteriae
✅ Answer: C
2. Vibrio cholerae is:
A. Gram-positive cocci
B. Gram-negative curved bacilli
C. Gram-positive bacilli
D. Acid-fast bacilli
✅ Answer: B
3. The main route of transmission of cholera is:
A. Airborne
B. Vector-borne
C. Fecal–oral
D. Sexual contact
✅ Answer: C
4. Cholera toxin causes diarrhea by increasing:
A. cGMP
B. cAMP
C. Calcium
D. ATP
✅ Answer: B
5. Cholera toxin is an example of:
A. Endotoxin
B. Neurotoxin
C. AB₅ exotoxin
D. Cytolysin
✅ Answer: C
6. The B subunit of cholera toxin binds to:
A. CD4 receptor
B. GM1 ganglioside
C. Toll-like receptor
D. Sodium channel
✅ Answer: B
7. The site of action of Vibrio cholerae is:
A. Stomach
B. Large intestine
C. Small intestine
D. Liver
✅ Answer: C
8. Stool in cholera is typically described as:
A. Bloody
B. Mucoid
C. Rice-water stool
D. Greenish
✅ Answer: C
9. Which feature is usually absent in cholera?
A. Profuse diarrhea
B. Dehydration
C. Fever
D. Vomiting
✅ Answer: C
10. Incubation period of cholera is usually:
A. 1–2 hours
B. 1–5 days
C. 7–14 days
D. 1 month
✅ Answer: B
11. Gold standard for diagnosis of cholera is:
A. Rapid antigen test
B. PCR
C. Culture
D. Serology
✅ Answer: C
12. Best enrichment medium for Vibrio cholerae is:
A. Selenite F broth
B. Alkaline peptone water
C. Nutrient broth
D. MacConkey broth
✅ Answer: B
13. Selective medium for isolation of Vibrio cholerae is:
A. Blood agar
B. MacConkey agar
C. TCBS agar
D. Lowenstein-Jensen
✅ Answer: C
14. Colonies of Vibrio cholerae on TCBS agar are:
A. Green
B. Colorless
C. Yellow
D. Black
✅ Answer: C
15. Vibrio cholerae is oxidase:
A. Negative
B. Positive
C. Variable
D. Weak
✅ Answer: B
16. Characteristic motility of Vibrio cholerae is:
A. Tumbling
B. Swarming
C. Darting
D. Non-motile
✅ Answer: C
17. Motility of Vibrio cholerae is inhibited by:
A. Antibiotics
B. Antisera
C. Heat
D. Acid
✅ Answer: B
18. The string test is positive in:
A. Shigella
B. Salmonella
C. Vibrio cholerae
D. Campylobacter
✅ Answer: C
19. Which serogroup is most commonly associated with epidemics?
A. O1
B. O2
C. O75
D. Non-O1
✅ Answer: A
20. Another epidemic serogroup of Vibrio cholerae is:
A. O55
B. O111
C. O139
D. O26
✅ Answer: C
21. Reservoir of Vibrio cholerae is mainly:
A. Animals
B. Soil
C. Humans
D. Insects
✅ Answer: C
22. Which factor increases susceptibility to cholera?
A. Hyperacidity
B. Achlorhydria
C. High immunity
D. Breastfeeding
✅ Answer: B
23. The diarrhea in cholera is due to:
A. Inflammation
B. Tissue invasion
C. Toxin-mediated secretion
D. Ulceration
✅ Answer: C
24. Which electrolyte loss causes muscle cramps in cholera?
A. Sodium
B. Potassium
C. Calcium
D. Magnesium
✅ Answer: B
25. Most common cause of death in untreated cholera is:
A. Sepsis
B. Renal failure
C. Hypovolemic shock
D. Perforation
✅ Answer: C
26. Best initial treatment for cholera is:
A. Antibiotics
B. Antidiarrheals
C. Oral rehydration therapy
D. Surgery
✅ Answer: C
27. Which solution is lifesaving in cholera?
A. Normal saline
B. ORS
C. Dextrose
D. Ringer lactate only
✅ Answer: B
28. Case fatality rate of cholera with proper treatment is:
A. >50%
B. 20–30%
C. <1%
D. 10%
✅ Answer: C
29. Rapid diagnostic tests for cholera detect:
A. Antibodies
B. Antigens
C. DNA only
D. Toxins only
✅ Answer: B
30. Best specimen for laboratory diagnosis is:
A. Blood
B. Urine
C. Stool
D. CSF
✅ Answer: C
31. Transport medium for stool sample in cholera is:
A. Amies
B. Cary-Blair
C. Stuart
D. Venkatraman medium
✅ Answer: B
32. Cholera is more common in:
A. Developed countries
B. Cold climates
C. Areas with poor sanitation
D. Desert regions
✅ Answer: C
33. Cholera shows seasonal increase during:
A. Winter
B. Rainy season
C. Snowfall
D. Autumn
✅ Answer: B
34. Asymptomatic carriers of cholera:
A. Do not spread disease
B. Spread disease
C. Are immune
D. Do not shed organisms
✅ Answer: B
35. Which is NOT a preventive measure for cholera?
A. Safe water
B. Sanitation
C. Hand hygiene
D. Steroids
✅ Answer: D
36. Oral cholera vaccine is useful in:
A. Endemic areas
B. Outbreak situations
C. High-risk populations
D. All of the above
✅ Answer: D
37. Public health importance of cholera includes:
A. Sporadic cases only
B. Slow transmission
C. Explosive outbreaks
D. No mortality
✅ Answer: C
38. Which food is commonly associated with cholera transmission?
A. Dairy products
B. Undercooked seafood
C. Fruits
D. Dry grains
✅ Answer: B
39. Cholera diarrhea is best classified as:
A. Inflammatory
B. Osmotic
C. Secretory
D. Malabsorptive
✅ Answer: C
40. Stool microscopy in cholera shows:
A. Pus cells
B. RBCs
C. No inflammatory cells
D. Parasites
✅ Answer: C
41. Vibrio cholerae ferments:
A. Lactose
B. Mannitol
C. Sucrose
D. Glucose only
✅ Answer: C
42. String test uses:
A. Bile salts
B. Sodium deoxycholate
C. Acetic acid
D. Formalin
✅ Answer: B
43. Cholera is a notifiable disease because:
A. High mortality
B. Epidemic potential
C. Zoonotic nature
D. Chronic carrier state
✅ Answer: B
44. Main aim of laboratory diagnosis during outbreaks is:
A. Cure patient
B. Confirm etiology
C. Identify resistance
D. Reduce symptoms
✅ Answer: B
45. Cholera toxin gene is carried by:
A. Plasmid
B. Bacteriophage
C. Chromosome only
D. Transposon
✅ Answer: B
46. Which biotype caused the 7th pandemic?
A. Classical
B. El Tor
C. O139
D. Non-O1
✅ Answer: B
47. Main preventive strategy for cholera control is:
A. Antibiotics
B. Vaccination only
C. Safe water and sanitation
D. Isolation only
✅ Answer: C
48. Cholera is best described as:
A. Invasive diarrhea
B. Inflammatory diarrhea
C. Non-inflammatory secretory diarrhea
D. Dysenteric diarrhea
✅ Answer: C
49. Which vitamin deficiency worsens dehydration outcome?
A. Vitamin A
B. Vitamin D
C. Vitamin B complex
D. Vitamin K
✅ Answer: C
50. Most effective single intervention to reduce cholera mortality is:
A. Antibiotics
B. ORS
C. Vaccination
D. Surveillance
✅ Answer: B