Introduction
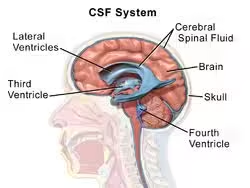
- Cerebrospinal fluid is a clear, colorless body fluid present in and around the central nervous system.
- It fills the ventricles of the brain, surrounds the brain and spinal cord in the subarachnoid space, and also occupies the central canal of the spinal cord.
- CSF is one of the most important protective fluids of the body because it acts as a cushion for delicate nervous tissue.
- It protects the brain and spinal cord from mechanical injury, helps in transport of nutrients, removes waste products, and maintains chemical stability of the nervous system.
- Because many diseases of the nervous system alter the composition of CSF, laboratory examination of CSF provides valuable diagnostic information.
Formation of Cerebrospinal Fluid
- CSF is mainly produced by the choroid plexus, a specialized vascular structure present in the ventricles of the brain.
- About 70% of CSF is formed by the choroid plexus.
- The remaining small amount is produced by:
- Ependymal lining of ventricles
- Brain capillaries
Sites of Formation
- Lateral ventricles
- Third ventricle
- Fourth ventricle
Daily Production
- About 500 mL per day
Total Volume
- Adult body normally contains 120–150 mL of CSF at any given time.
Circulation of CSF
- CSF formed in the lateral ventricles passes through:
- Interventricular foramina
- Third ventricle
- Cerebral aqueduct
- Fourth ventricle
- From the fourth ventricle it enters:
- Subarachnoid space
- Central canal of spinal cord
Absorption
- CSF is absorbed into venous circulation through arachnoid villi.
Choroid plexus plays the major role in CSF formation.
Functions of CSF
1. Mechanical Protection
- CSF acts as a shock absorber and cushions the brain and spinal cord against sudden movements or external injury.
- It protects delicate nervous tissue from trauma.
2. Buoyancy of Brain
- The brain has considerable weight, but when suspended in CSF its effective weight is greatly reduced.
- This prevents pressure on the lower parts of the brain.
3. Maintenance of Intracranial Pressure
- CSF helps maintain constant pressure inside the skull and spinal canal.
4. Transport of Nutrients
- CSF carries glucose, electrolytes, and other nutrients required by brain cells.
5. Removal of Waste Products
- Metabolic waste products from brain tissue are removed through CSF circulation.
6. Chemical Stability
- CSF maintains proper ionic balance around neurons, which is essential for nerve impulse conduction.
7. Medium for Exchange
- Acts as a medium for exchange of substances between blood and nervous tissue.
8. Defense Function
- Helps protect central nervous system by diluting harmful substances and participating in immune surveillance.
Collection of Cerebrospinal Fluid
- Collection of Cerebrospinal fluid is an important diagnostic procedure used to examine diseases of the central nervous system.
- CSF is collected mainly for:
- Chemical examination
- Microscopic examination
- Microbiological examination
- Pressure measurement
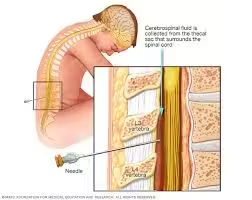
- The most common method of collection is lumbar puncture.
Method of Collection
Lumbar Puncture
- Lumbar puncture is the standard method used for CSF collection.
- A sterile needle is introduced into the subarachnoid space of the lumbar region.
Site of Collection
Common Site
- Between L3–L4 vertebrae
- Between L4–L5 vertebrae
Reason
- Spinal cord ends above this level, so risk of injury is minimal.
Position of Patient
Lateral Position
- Patient lies on side with knees flexed toward chest.
Sitting Position
- Sometimes used when required.
Procedure
| Step | Procedure |
|---|---|
| 1 | Clean puncture site with antiseptic |
| 2 | Use sterile lumbar puncture needle |
| 3 | Insert needle in lumbar space |
| 4 | Collect CSF in sterile tubes |
| 5 | Withdraw needle carefully |
Number of Tubes Collected
Usually Three Tubes
- Tube 1 → Chemical examination
- Tube 2 → Microbiological examination
- Tube 3 → Cell count and microscopy
Amount Collected
- Usually 2–3 mL per tube
- Total 5–10 mL depending on requirement
Post-Procedure Care
- Monitor the Patient: The patient is usually observed for 1–2 hours after the procedure, particularly for any signs of complications like headache, bleeding, or neurological changes.
- Post-Lumbar Puncture Headache: A common side effect caused by a leak of CSF through the puncture site. It can typically be managed with bed rest, hydration, caffeine, and analgesics. In severe cases, a blood patch may be needed.
Potential Complications
- Post-Lumbar Puncture Headache: Occurs in about 10-30% of patients.
- Back Pain: Temporary pain at the site of the needle insertion.
- Bleeding: Rare but may occur, particularly in patients with bleeding disorders.
- Infection: Though rare, introducing infection into the spinal canal (meningitis) is a serious concern.
- Brain Herniation: If a patient has elevated intracranial pressure due to a mass lesion, herniation of the brainstem through the foramen magnum can occur.
Laboratory Examination of CSF
Physical examination
Colour and Clarity
- Normal CSF: Clear and colourless, resembling water.
- Abnormal Colors:
- Turbid or cloudy: Indicates an elevated number of cells (pleocytosis), commonly seen in infections such as bacterial meningitis or in cases of a high protein content.
- Xanthochromia (yellowish discolouration): Results from the breakdown of blood in the CSF.
- Pink/red (bloody): Suggests the presence of red blood cells. This can be due to a traumatic tap or a subarachnoid haemorrhage.
- Oily appearance: when fatty substances are present.
Appearance
Normal Appearance
- Fresh CSF is clear, transparent, and colorless.
Turbid CSF
- Indicates increased cells, bacteria, or protein.
Causes of Turbidity
- Bacterial meningitis
- High leukocyte count
- Severe protein increase
Turbidity or Cloudiness
- Normal CSF is crystal clear.
- Turbid CSF suggests the presence of white blood cells, red blood cells, bacteria, or fungi.
- Infections: Bacterial meningitis commonly causes a turbid appearance due to many white blood cells. Tuberculous or fungal meningitis may also cause turbidity, but often to a lesser degree.
- Increased Protein: Conditions like Guillain-Barré syndrome or tumours may cause CSF to appear turbid due to the accumulation of high levels of proteins.
- Lipids: Sometimes seen in cases of increased lipids in the blood or after fat embolism.
Viscosity
- Normal CSF is slightly more viscous than water but flows easily from the needle during a lumbar puncture.
- Increased viscosity is rare but can occur in conditions like metastatic mucinous tumours or rarely in hypoproteinaemia states.
Presence of Coagulum or Clot
- Normal CSF does not clot.
- Abnormal coagulation in the CSF may occur when there is an increased amount of fibrinogen or protein, which can be seen in:
- Tuberculous meningitis: CSF may form a fibrin web or clot when allowed to sit in a test tube. This is highly suggestive of tuberculous or fungal meningitis.
- Traumatic tap: Clotting may occur due to blood contamination from the procedure.
Opening Pressure
- Normal CSF pressure ranges from 6 to 20 cm H₂O (measured with the patient in a lateral decubitus position).
- Increased opening pressure May suggest conditions such as:
- Meningitis (particularly bacterial).
- Subarachnoid haemorrhage.
- Cerebral oedema.
- Tumors or space-occupying lesions.
- Idiopathic intracranial hypertension.
- Decreased opening pressure May occur in conditions such as:
- CSF leak (post-surgery, trauma, or spontaneous).
- Dehydration.
- CNS hypotension.
- Increased opening pressure May suggest conditions such as:
Chemical Analysis of CSF
Glucose
Principle
- Glucose in Cerebrospinal fluid is commonly estimated by the glucose oxidase–peroxidase method.
- Glucose is oxidized by glucose oxidase to form gluconic acid and hydrogen peroxide.
- Hydrogen peroxide reacts with chromogen in presence of peroxidase to produce a colored compound.
- The intensity of color formed is proportional to glucose concentration.
Procedure
| Tube | Working Reagent | Sample / Standard | Distilled Water |
|---|---|---|---|
| Blank | 1.0 mL | — | 0.01 mL |
| Standard | 1.0 mL | 0.01 mL glucose standard | — |
| Test | 1.0 mL | 0.01 mL CSF | — |
Observation
- A colored solution develops.
- Greater color intensity indicates higher glucose concentration.
Normal Value
- 50–80 mg/dL
- Usually about two-thirds of blood glucose level.
Clinical significance
- CSF glucose reflects blood glucose and brain metabolism.
Decreased Glucose Seen In
- Bacterial meningitis
- Tuberculous meningitis
- Fungal infection
Increased Glucose Seen In
- Diabetes mellitus
Protein
Principle
- Protein in CSF is commonly estimated by the sulfosalicylic acid method or turbidimetric method.
- Sulfosalicylic acid precipitates protein present in CSF, producing turbidity.
- The degree of turbidity is proportional to protein concentration.
Procedure
| Step | Procedure |
|---|---|
| 1 | Take 1 mL CSF in a clean test tube |
| 2 | Add 1 mL of 3% sulfosalicylic acid |
| 3 | Mix gently |
| 4 | Observe turbidity against light |
Observation
- Turbidity develops if protein is present.
- Greater turbidity indicates increased protein.
Normal Value
- 15–45 mg/dL
Clinical Significance
- CSF protein is lower than plasma protein because only small amounts normally pass through the blood-brain barrier.
Increased Protein Seen In
- Meningitis
- Brain tumors
- Multiple sclerosis
- Guillain-Barré syndrome
Decreased Protein
- Rare, usually after repeated lumbar puncture
Lactate
Principle
- Lactate present in CSF reacts enzymatically to produce a colored compound.
- The color intensity produced is directly proportional to lactate concentration.
Procedure
| Tube | Working Reagent | Sample / Standard |
|---|---|---|
| Test | 1.0 mL | 0.1 mL CSF |
| Standard | 1.0 mL | 0.1 mL lactate standard |
Steps
- Label test tubes as Test and Standard.
- Add 1.0 mL lactate reagent to both tubes.
- Add 0.1 mL CSF sample to test tube.
- Add 0.1 mL lactate standard to standard tube.
- Mix gently.
- Incubate for recommended time.
- Measure absorbance using colorimeter.
Observation
- Colored solution develops.
- Higher color intensity indicates increased lactate.
Normal Range
1.2-2.1 mmol/L.
Abnormal Findings
- Increased Lactate:
- Bacterial Meningitis: High levels of lactate (>3.5 mmol/L) indicate bacterial infection due to the anaerobic metabolism of the invading organisms and impaired oxygenation in the inflamed tissues.
- Fungal and Tuberculous Meningitis: Moderate increases in lactate can be seen.
- Stroke: Elevated lactate may indicate areas of ischemia or reduced oxygen supply to the brain.
- Normal or Slightly Increased Lactate:
- Viral Meningitis: Lactate levels are usually normal or only slightly elevated in viral infections.
Significance
- Lactate is particularly useful in distinguishing between bacterial and viral meningitis.
- High levels strongly suggest a bacterial cause, which requires more aggressive treatment.
Chloride
Principle
- Chloride in CSF reacts with silver nitrate to form silver chloride precipitate.
- The amount of chloride is measured by titration or colorimetric method.
Procedure
| Step | Procedure |
|---|---|
| 1 | Take 1 mL CSF sample in a clean test tube |
| 2 | Add few drops of potassium chromate indicator |
| 3 | Titrate with silver nitrate solution |
| 4 | Continue till brick-red endpoint appears |
Observation
- White precipitate forms first.
- Endpoint appears as brick-red color.
Normal Range
110-130 mEq/L.
Abnormal Findings
- Decreased Chloride:
- Tuberculous Meningitis: Chloride levels are often reduced in TB meningitis.
- Other Infections: Prolonged bacterial or fungal infections may also lower CSF chloride, though it is not a commonly measured parameter today.
Significance
- Chloride levels are rarely used as a primary diagnostic tool in modern practice, as more specific and sensitive markers (such as glucose and lactate) are preferred.
Cellular Examination (Cytology)
Cell Count: Normal CSF contains very few cells (0–5 white blood cells/µL). Increased white blood cell count (pleocytosis) indicates infection, inflammation, or malignancy.
- Neutrophils: High in bacterial meningitis.
- Lymphocytes: Predominant in viral, fungal, or tuberculous meningitis and autoimmune conditions.
Red Blood Cells (RBCs): RBCs can indicate bleeding (e.g., subarachnoid haemorrhage) or trauma during a lumbar puncture.
Microbiological Examination
1. Direct Microscopic Examination
Gram Staining
- A drop of centrifuged CSF sediment is stained by Gram stain.
- Helps detect bacteria immediately.
Acid-Fast Staining
- Used when tuberculous meningitis is suspected.
India Ink Preparation
- Used for fungal infection, especially cryptococcus.
2. Culture Examination
Principle
- CSF is inoculated onto culture media to isolate microorganisms.
Common Media Used
- Blood agar
- Chocolate agar
- MacConkey agar
Incubation
- Incubate at 37°C
3. Common Organisms Detected
- Neisseria meningitidis
- Streptococcus pneumoniae
- Mycobacterium tuberculosis
4. Sensitivity Testing
- Performed after culture to select effective antibiotics.
Serological and Immunological Tests
- Antibody Detection: Useful for diagnosing neurosyphilis or autoimmune diseases.
- Antigen Detection: Helpful in diagnosing specific pathogens (e.g., Cryptococcal antigen in fungal meningitis).
Other Special Tests
- Beta-2 transferrin: A specific marker for CSF, useful in diagnosing CSF leaks.
- Tau Protein and Amyloid Beta: Used to diagnose neurodegenerative diseases like Alzheimer’s.
Clinical Significance
1. Diagnosis of Meningitis
- CSF examination is essential for diagnosing Meningitis.
- In meningitis:
- Protein level increases
- Glucose level decreases
- Cell count rises
2. Differentiation of Types of Meningitis
- CSF helps distinguish:
- Bacterial meningitis → high neutrophils, low glucose, high protein
- Viral meningitis → lymphocytes predominate, glucose usually normal
- Tuberculous meningitis → high protein, low chloride, cobweb clot formation
3. Detection of Central Nervous System Infections
- Microbiological examination detects bacteria, fungi, and other pathogens directly from CSF.
4. Diagnosis of Hemorrhage
- Presence of blood or xanthochromia suggests Subarachnoid hemorrhage.
5. Evaluation of Neurological Disorders
- Increased protein may occur in:
- Demyelinating diseases
- Peripheral neuropathies
- Nerve root lesions
6. Detection of Raised Intracranial Pressure
- CSF pressure measurement helps identify intracranial hypertension.
7. Monitoring Disease Progress and Treatment
- Repeated CSF examination helps assess treatment response in infections and neurological diseases.
8. Detection of Malignant Cells
- CSF may show malignant cells in meningeal spread of tumors.