
Introduction
-
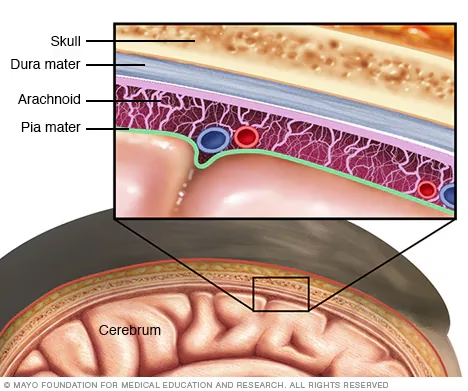
Meningitis is a serious inflammatory condition involving the meninges, the protective membranes covering the brain and spinal cord.
-
It is a medical emergency, especially in cases of bacterial meningitis, due to its rapid progression and high mortality rate.
-
The disease can affect individuals of all age groups, with neonates, children, the elderly, and immunocompromised patients being at higher risk.
-
Meningitis may be caused by bacterial, viral, fungal, or parasitic pathogens, each with different clinical severity and outcomes.
-
If not diagnosed and treated promptly, meningitis can lead to severe complications such as seizures, hearing loss, neurological deficits, coma, or death.
-
Early and accurate diagnosis is essential to initiate appropriate therapy and reduce morbidity and mortality.
-
Laboratory investigations, particularly cerebrospinal fluid (CSF) analysis, play a central role in confirming the diagnosis.
Symptoms
A. General Symptoms
-
High-grade fever
-
Severe headache
-
Nausea and vomiting
-
Fatigue and malaise
-
Photophobia (sensitivity to light)
B. Classical Signs (Triad)
-
Fever
-
Neck stiffness (nuchal rigidity)
-
Altered mental status (confusion, drowsiness)
C. Neurological Symptoms
-
Confusion or disorientation
-
Seizures
-
Altered consciousness or coma
-
Difficulty concentrating
-
Focal neurological deficits
D. Symptoms in Infants and Children
-
High-pitched cry
-
Poor feeding
-
Bulging fontanelle
-
Irritability or lethargy
-
Vomiting
-
Seizures
Causes
A. Infectious Causes
1. Bacterial Causes
-
Streptococcus pneumoniae
-
Neisseria meningitidis
-
Haemophilus influenzae type b
-
Listeria monocytogenes
-
Group B Streptococcus
2. Viral Causes
-
Enteroviruses
-
Herpes simplex virus (HSV)
-
Varicella-zoster virus (VZV)
-
Cytomegalovirus (CMV)
3. Fungal Causes
-
Cryptococcus neoformans
-
Histoplasma capsulatum
4. Parasitic Causes
-
Naegleria fowleri
-
Toxoplasma gondii
B. Non-Infectious Causes
-
Autoimmune diseases
-
Certain medications
-
Malignancies
-
Head trauma or neurosurgical procedures
Risk Factors
-
Age (infants, young children, elderly)
-
Immunocompromised state (HIV/AIDS, cancer, transplant patients)
-
Lack of vaccination
-
Crowded living conditions (hostels, dormitories)
-
Recent infections (sinusitis, otitis media)
-
Pregnancy (risk of Listeria infection)
-
Chronic diseases (diabetes, liver disease)
-
Head injury or neurosurgery
-
Exposure to contaminated water (for parasitic meningitis)
Complications of Meningitis
A. Neurological Complications
-
Hearing loss
-
Seizure disorders
-
Cognitive impairment
-
Memory loss
-
Motor deficits
-
Hydrocephalus
B. Systemic Complications
-
Septic shock
-
Disseminated intravascular coagulation (DIC)
-
Multi-organ failure
C. Long-Term Complications
-
Learning disabilities
-
Behavioral problems
-
Speech and vision impairment
-
Permanent neurological damage
D. Fatal Outcome
-
Untreated or severe meningitis can lead to coma and death
Types of Meningitis and Common Pathogens
1. Bacterial Meningitis
Bacterial meningitis is the most severe and life-threatening form, requiring immediate medical intervention.
Common Pathogens:
-
Streptococcus pneumoniae
-
Leading cause of bacterial meningitis in both adults and children
-
Associated with high mortality and neurological complications
-
-
Neisseria meningitidis
-
Commonly causes epidemics and outbreaks
-
Frequently seen in crowded environments such as dormitories, hostels, and military camps
-
-
Haemophilus influenzae type b (Hib)
-
Previously a major cause in children
-
Incidence significantly reduced due to widespread vaccination
-
-
Listeria monocytogenes
-
Affects neonates, elderly, pregnant women, and immunocompromised individuals
-
Transmitted mainly through contaminated food
-
-
Group B Streptococcus (Streptococcus agalactiae)
-
Common cause of neonatal meningitis
-
Transmitted from mother to newborn during childbirth
-
2. Viral Meningitis
Viral meningitis is generally less severe and often self-limiting compared to bacterial meningitis.
Common Pathogens:
-
Enteroviruses
-
Most frequent cause of viral meningitis
-
Predominantly affects children
-
-
Herpes simplex virus (HSV-2 > HSV-1)
-
Can cause recurrent meningitis
-
Associated with severe neurological complications in some cases
-
-
Varicella-zoster virus (VZV)
-
Can cause meningitis, especially in elderly or immunocompromised individuals
-
-
Cytomegalovirus (CMV)
-
Seen mainly in immunocompromised patients, including transplant recipients and HIV-infected individuals
-
3. Fungal Meningitis
Fungal meningitis occurs primarily in immunocompromised hosts and usually has a chronic course.
Common Pathogens:
-
Cryptococcus neoformans
-
Most common cause of fungal meningitis
-
Frequently affects patients with HIV/AIDS
-
-
Histoplasma capsulatum
-
Causes meningitis in endemic regions
-
Often associated with chronic infection
-
4. Parasitic Meningitis
Parasitic meningitis is rare but often fatal, requiring rapid diagnosis and management.
Common Pathogens:
-
Naegleria fowleri
-
Causes primary amoebic meningoencephalitis
-
Acquired from contaminated freshwater
-
Rapidly progressive and usually fatal
-
-
Toxoplasma gondii
-
Causes meningitis or meningoencephalitis in immunocompromised individuals
-
Commonly seen in HIV/AIDS patients
-
Sample Collection
Cerebrospinal Fluid (CSF)
-
Cerebrospinal fluid (CSF) analysis is the cornerstone of meningitis diagnosis, as it directly reflects pathological changes occurring in the meninges.
-
CSF is obtained by lumbar puncture, which allows safe access to the subarachnoid space.
Procedure of Lumbar Puncture
-
Positioning:
-
The patient may be seated with legs hanging off the table and the spine flexed, or
-
Positioned in the lateral decubitus position with knees drawn up to the chest to widen the intervertebral spaces.
-
-
Site Selection:
-
The puncture is performed at the L3–L4 or L4–L5 intervertebral space to avoid injury to the spinal cord.
-
-
Sterile Technique:
-
Strict aseptic precautions are essential to prevent contamination and secondary infection.
-
-
Collection:
-
CSF is collected in sterile, labeled tubes.
-
The first tube is reserved for microbiological examination (Gram stain, culture, PCR).
-
-
Volume:
-
A total of 10–20 mL of CSF is usually sufficient for:
-
Microbiological tests
-
Biochemical analysis
-
Cytological examination
-
-
Blood Cultures
-
Blood cultures are commonly collected at the same time as lumbar puncture.
-
They are crucial for detecting bacteremia, which often accompanies bacterial meningitis.
-
At least two blood culture samples should be obtained.
-
Samples should be drawn from different venipuncture sites to increase diagnostic yield and reduce contamination.
-
Blood cultures may be positive even when CSF cultures are negative, especially if antibiotics have been started.
Other Specimens (When Indicated)
Depending on clinical suspicion and patient presentation, additional specimens may be collected:
-
Urine:
-
Used for viral PCR testing, particularly in suspected viral meningitis.
-
-
Throat Swabs:
-
Helpful for rapid antigen detection of viral pathogens.
-
-
Vesicular Fluid:
-
Collected in patients with vesicular skin lesions when herpes simplex virus (HSV) or varicella-zoster virus (VZV) infection is suspected.
-
Laboratory Diagnosis
1. Cerebrospinal Fluid (CSF) Examination
A. Physical Examination
-
Appearance:
-
Normal CSF is clear and colorless
-
Turbid or cloudy CSF suggests bacterial or fungal infection
-
-
Color:
-
Xanthochromia (yellowish CSF) may indicate hemorrhage or high protein levels
-
B. Chemical Analysis
-
Protein:
-
Elevated in bacterial and fungal meningitis
-
Normal or mildly increased in viral meningitis
-
-
Glucose:
-
Decreased in bacterial and fungal meningitis
-
Usually normal in viral meningitis
-
-
Lactate:
-
Increased in bacterial meningitis due to anaerobic metabolism
-
C. Cell Count and Differential
-
Total WBC count: Increased in meningitis
-
Bacterial meningitis:
-
Usually >1000 cells/mm³
-
Predominantly neutrophils
-
-
Viral meningitis:
-
Usually <500 cells/mm³
-
Predominantly lymphocytes
-
-
Fungal/Tubercular meningitis:
-
Lymphocytic predominance
-
2. Microscopic Examination
-
Gram Stain:
-
Rapid and simple test
-
Positive in 60–90% of untreated bacterial meningitis cases
-
-
India Ink Preparation:
-
Used for detection of Cryptococcus neoformans
-
-
Acid-Fast Stain:
-
Used when tubercular meningitis is suspected
-
3. Culture Methods
A. Bacterial Culture
-
CSF inoculated onto:
-
Blood agar
-
Chocolate agar
-
Thayer–Martin agar (for Neisseria meningitidis)
-
-
Incubation at 35–37°C with CO₂
-
Helps in:
-
Confirming diagnosis
-
Antibiotic susceptibility testing
-
B. Fungal Culture
-
Cultured on Sabouraud dextrose agar
-
Requires prolonged incubation
-
Useful for chronic meningitis
4. Molecular Methods
A. Polymerase Chain Reaction (PCR)
-
Highly sensitive and specific
-
Rapid detection of pathogens
-
Particularly useful for:
-
Viral meningitis (enteroviruses, HSV)
-
Culture-negative bacterial meningitis
-
-
Multiplex PCR can detect multiple pathogens simultaneously
B. Nucleic Acid Hybridization
-
Fluorescent In Situ Hybridization (FISH)
-
Useful in:
-
Polymicrobial infections
-
Cases with prior antibiotic therapy
-
5. Serological Tests
-
Antigen detection tests:
-
Useful for certain viral and bacterial pathogens
-
-
Antibody detection:
-
Helpful in selected cases, especially when culture is negative
-
More useful for retrospective diagnosis
-
6. Blood Investigations
-
Blood cultures:
-
Often positive in bacterial meningitis
-
-
Complete blood count (CBC):
-
Leukocytosis common in bacterial meningitis
-
-
Inflammatory markers:
-
CRP and procalcitonin may be elevated
-
7. Imaging Studies (Supportive Role)
-
CT or MRI brain:
-
Performed before lumbar puncture if raised intracranial pressure is suspected
-
Helps rule out mass lesions or cerebral edema
-
Clinical Considerations
1. Rapid Diagnosis and Early Treatment
-
Meningitis is a medical emergency.
-
Empirical treatment should be started immediately after sample collection, without waiting for laboratory confirmation.
-
Delay in therapy significantly increases mortality and morbidity, especially in bacterial meningitis.
2. Empirical Therapy
-
Initial treatment is based on:
-
Age of the patient
-
Clinical severity
-
Likely causative organisms
-
-
Common empirical regimen for suspected bacterial meningitis includes:
-
Broad-spectrum intravenous antibiotics (e.g., ceftriaxone and vancomycin)
-
Ampicillin added in neonates and elderly to cover Listeria monocytogenes
-
-
Corticosteroids (e.g., dexamethasone) may be administered to reduce inflammatory complications and neurological sequelae.
3. Importance of Timing
-
Antibiotics should ideally be given after CSF and blood samples are collected.
-
However, treatment should not be delayed if lumbar puncture is contraindicated or delayed.
4. Interpretation of Laboratory Results
-
Laboratory results must be correlated with:
-
Clinical signs (fever, neck stiffness, altered sensorium)
-
Epidemiological factors
-
Vaccination status
-
-
Normal CSF findings do not always exclude meningitis, particularly early in the disease.
5. Follow-Up and Monitoring
-
Clinical response should be closely monitored.
-
Follow-up lumbar puncture may be required in:
-
Poor response to therapy
-
Fungal or tubercular meningitis
-
Persistent or worsening neurological symptoms
-
6. Infection Control and Public Health Measures
-
Suspected meningococcal meningitis requires:
-
Isolation of the patient
-
Chemoprophylaxis for close contacts
-
-
Notification to public health authorities may be required in outbreak situations.
7. Special Patient Populations
-
Neonates:
-
Higher risk of complications
-
Different causative organisms
-
-
Elderly and immunocompromised patients:
-
Atypical presentation
-
Higher likelihood of fungal or opportunistic infections
-
-
Pregnant women:
-
Increased risk of Listeria infection
-
8. Prognostic Factors
-
Early diagnosis and treatment improve outcomes.
-
Poor prognostic indicators include:
-
Delayed therapy
-
Altered consciousness at presentation
-
High CSF protein and low glucose
-
Presence of septic shock
-
MCQs
1. Meningitis is defined as inflammation of:
A. Brain parenchyma
B. Spinal cord
C. Meninges
D. Ventricles
Answer: C
2. The most life-threatening form of meningitis is:
A. Viral
B. Fungal
C. Parasitic
D. Bacterial
Answer: D
3. The leading cause of bacterial meningitis in adults is:
A. Neisseria meningitidis
B. Streptococcus pneumoniae
C. Haemophilus influenzae
D. Listeria monocytogenes
Answer: B
4. Meningitis outbreaks in crowded places are commonly caused by:
A. Streptococcus pneumoniae
B. Haemophilus influenzae
C. Neisseria meningitidis
D. Listeria monocytogenes
Answer: C
5. Group B Streptococcus commonly causes meningitis in:
A. Adults
B. Elderly
C. Neonates
D. Immunocompromised
Answer: C
6. Most common cause of viral meningitis is:
A. HSV
B. CMV
C. Enteroviruses
D. VZV
Answer: C
7. HSV-2 meningitis is associated with:
A. Mild illness only
B. Severe neurological complications
C. Skin rash only
D. Asymptomatic infection
Answer: B
8. The most common cause of fungal meningitis in HIV patients is:
A. Candida albicans
B. Histoplasma capsulatum
C. Cryptococcus neoformans
D. Aspergillus fumigatus
Answer: C
9. Naegleria fowleri causes:
A. Viral meningitis
B. Chronic meningitis
C. Primary amoebic meningoencephalitis
D. Tubercular meningitis
Answer: C
10. The cornerstone of meningitis diagnosis is:
A. Blood culture
B. Imaging
C. CSF analysis
D. Serology
Answer: C
11. CSF is collected by:
A. Venipuncture
B. Bone marrow aspiration
C. Lumbar puncture
D. Ventricular tap
Answer: C
12. Safe lumbar puncture site is:
A. L1–L2
B. L2–L3
C. L3–L4
D. T12–L1
Answer: C
13. CSF should be collected using:
A. Clean technique
B. Aseptic technique
C. No precautions
D. Alcohol cleaning only
Answer: B
14. First CSF tube is used for:
A. Biochemistry
B. Cytology
C. Microbiology
D. Serology
Answer: C
15. Normal appearance of CSF is:
A. Turbid
B. Cloudy
C. Clear and colorless
D. Yellow
Answer: C
16. Turbid CSF suggests:
A. Viral meningitis
B. Normal CSF
C. Bacterial/fungal meningitis
D. Hemorrhage only
Answer: C
17. CSF glucose is typically low in:
A. Viral meningitis
B. Bacterial meningitis
C. Normal CSF
D. Migraine
Answer: B
18. Normal CSF glucose is approximately:
A. Equal to serum glucose
B. 10% of serum glucose
C. 2/3 of serum glucose
D. Zero
Answer: C
19. Predominant cells in bacterial meningitis CSF are:
A. Lymphocytes
B. Monocytes
C. Neutrophils
D. Eosinophils
Answer: C
20. Predominant cells in viral meningitis CSF are:
A. Neutrophils
B. Lymphocytes
C. Eosinophils
D. Basophils
Answer: B
21. CSF protein is markedly increased in:
A. Viral meningitis
B. Bacterial meningitis
C. Migraine
D. Tension headache
Answer: B
22. Gram stain positivity in untreated bacterial meningitis is:
A. <10%
B. 20–30%
C. 60–90%
D. 100%
Answer: C
23. India ink preparation is used to detect:
A. Neisseria
B. HSV
C. Cryptococcus
D. Enterovirus
Answer: C
24. Culture medium for Neisseria meningitidis is:
A. MacConkey agar
B. Blood agar
C. Chocolate agar
D. Thayer-Martin agar
Answer: D
25. Fungal meningitis culture is done on:
A. Blood agar
B. Lowenstein-Jensen
C. Sabouraud dextrose agar
D. TCBS agar
Answer: C
26. PCR is most useful for diagnosis of:
A. Parasitic meningitis
B. Viral meningitis
C. Chemical meningitis
D. Drug-induced meningitis
Answer: B
27. Advantage of PCR is:
A. Low sensitivity
B. Slow results
C. High sensitivity and specificity
D. Requires live organisms
Answer: C
28. Blood cultures are especially important in:
A. Viral meningitis
B. Fungal meningitis
C. Bacterial meningitis
D. Migraine
Answer: C
29. Minimum number of blood cultures recommended is:
A. One
B. Two
C. Three
D. Four
Answer: B
30. Imaging before lumbar puncture is required when there is:
A. Fever only
B. Headache only
C. Raised intracranial pressure
D. Mild meningitis
Answer: C
31. CT/MRI before LP is done to prevent:
A. Infection
B. Bleeding
C. Brain herniation
D. Pain
Answer: C
32. Normal CSF WBC count is:
A. 0–5 cells/mm³
B. 10–50 cells/mm³
C. 100–500 cells/mm³
D. >1000 cells/mm³
Answer: A
33. Elevated CSF lactate suggests:
A. Viral meningitis
B. Bacterial meningitis
C. Migraine
D. Normal CSF
Answer: B
34. Eosinophils in CSF suggest:
A. Viral meningitis
B. Bacterial meningitis
C. Parasitic meningitis
D. Fungal meningitis
Answer: C
35. Empirical treatment should be started:
A. After culture report
B. After PCR result
C. Immediately after sample collection
D. After imaging only
Answer: C
36. First-line empirical therapy for bacterial meningitis includes:
A. Penicillin only
B. Ceftriaxone + vancomycin
C. Acyclovir only
D. Amphotericin B
Answer: B
37. Dexamethasone is given to:
A. Kill bacteria
B. Reduce inflammation
C. Increase CSF glucose
D. Improve culture growth
Answer: B
38. Follow-up lumbar puncture is indicated in:
A. All patients
B. Poor clinical response
C. Viral meningitis only
D. Migraine
Answer: B
39. Meningococcal meningitis requires:
A. No isolation
B. Public health notification
C. Surgery
D. Chemotherapy
Answer: B
40. Close contacts of meningococcal meningitis require:
A. Vaccination only
B. Chemoprophylaxis
C. No treatment
D. Surgery
Answer: B
41. Poor prognostic factor in meningitis is:
A. Early treatment
B. Normal consciousness
C. Delayed therapy
D. Mild headache
Answer: C
42. Listeria meningitis is common in:
A. Teenagers
B. Healthy adults
C. Elderly and neonates
D. Athletes
Answer: C
43. CMV meningitis occurs mainly in:
A. Healthy adults
B. Children
C. Immunocompromised
D. Neonates only
Answer: C
44. Clear CSF with lymphocytes and normal glucose suggests:
A. Bacterial meningitis
B. Viral meningitis
C. Fungal meningitis
D. Subarachnoid hemorrhage
Answer: B
45. Gold standard for definitive diagnosis of meningitis is:
A. Clinical signs
B. Imaging
C. Culture of CSF
D. CBC
Answer: C
46. Lumbar puncture is contraindicated in:
A. Fever
B. Headache
C. Raised intracranial pressure
D. Neck stiffness
Answer: C
47. Primary goal of laboratory diagnosis is to:
A. Reduce cost
B. Identify pathogen
C. Delay treatment
D. Avoid lumbar puncture
Answer: B
48. Early diagnosis of meningitis helps prevent:
A. Fever
B. Headache
C. Neurological complications
D. Vomiting
Answer: C
49. Most important specimen in meningitis diagnosis is:
A. Urine
B. Blood
C. CSF
D. Throat swab
Answer: C
50. Meningitis management requires:
A. Laboratory diagnosis only
B. Clinical diagnosis only
C. Integrated clinical and laboratory approach
D. Imaging alone
Answer: C